Part 7: Post-operative Radiographs
ASSESSMENT OF POST-OPERATIVE RADIOGRAPHS
Serial radiographs are often performed 24 to 48 hours post op, at 6 weeks and possibly other intervals in the first year post surgery. Joint replacements may require imaging annually.
Metalware and/or prosthesis should be imaged in at least two planes to evaluate anatomical alignment and should extend beyond the hardware to allow adjacent soft tissues, bones, and cement restrictors to be reviewed.
Radiological assessment may include the following:
Union of osteotomy or arthrodesis
- Mal-union: union in a suboptimal position
- Non-union: confirmed failure of osseous union at least 6 months after surgery
- CT imaging is very helpful to confirm bony union
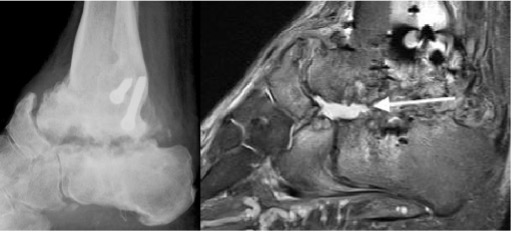
Infected nonunion subtalar joint (arrow)
Incorporation of bone graft
Anatomical alignment

Subluxation of failed total ankle replacement
Metalware loosening
Radiographic signs of chronic low-grade infection may be identical to mechanical aseptic loosening including periprosthetic lucency, subsidence and periosteal reaction.
Comparison with prior radiographs is important to assess for progression of changes that may indicate hardware failure.
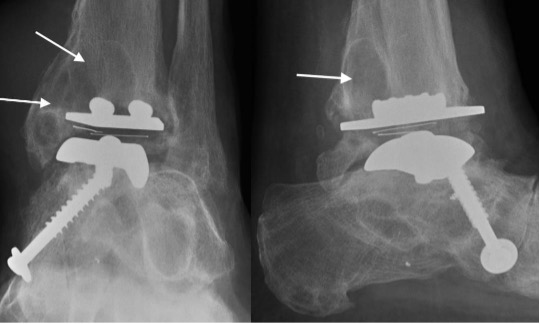
Failing TAR with progressive periprosthetic lucency (arrows)
Metalware failure

Screw fracture (arrow)
Infection
Avascular necrosis
- Increased sclerosis as new bone is laid down over necrotic trabeculae
- Necrotic region becomes sharply demarcated due resorption of surrounding vascularised bone
- A ‘crescent sign’ representing a linear subchondral fracture, secondary to collapse of the necrotic area, may be seen in the talus and distal tibia but is less common in the small bones of the foot
- End-stage findings include flattening, collapse and fragmentation of the articular surface and development of secondary osteoarthritis
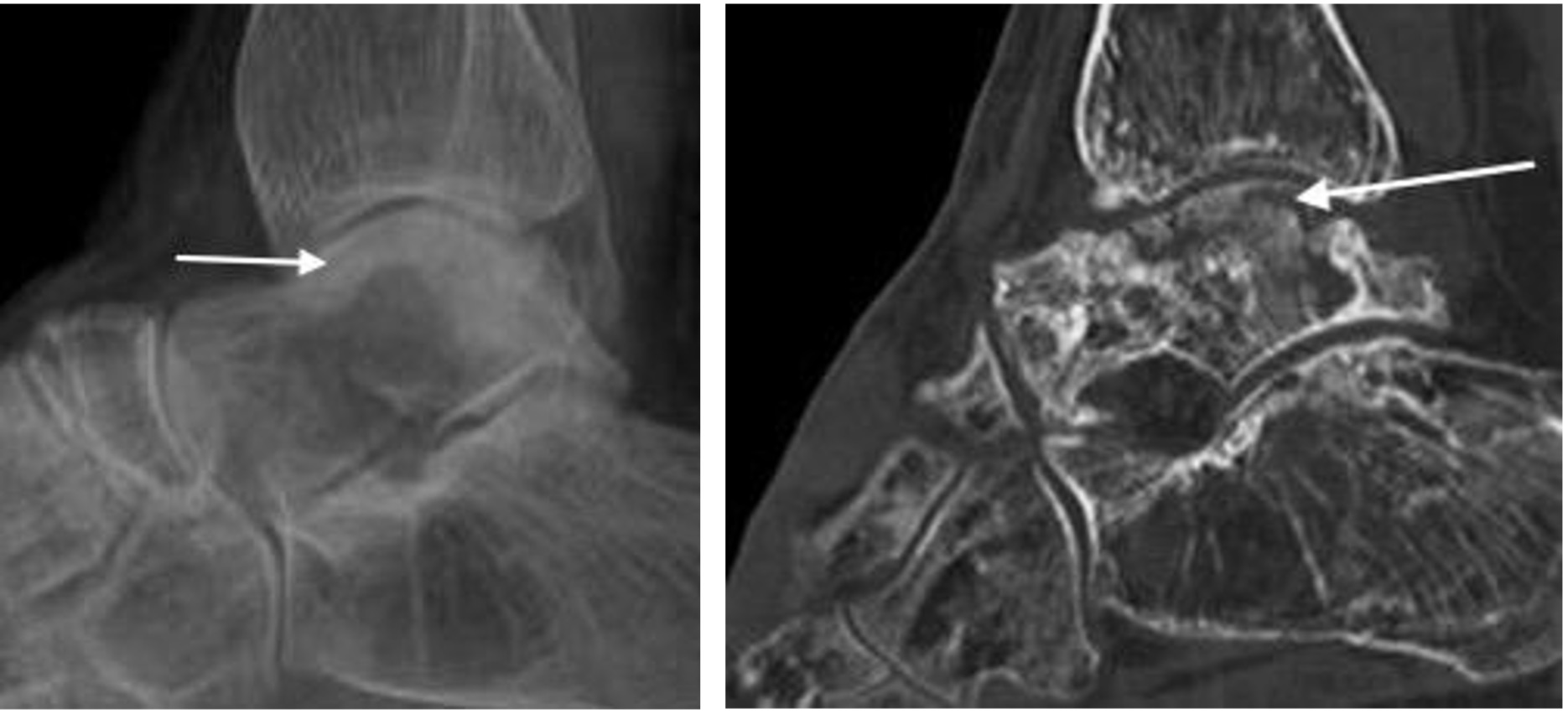
Avascular necrosis of the alar dome following talar neck fracture with subchondral sclerosis and fracture (arrows). Note disuse osteopaenia.