The Cavovarus Foot
Definition
- The cavovarus foot is a foot with a high arch that maintains its position on weight bearing.
- Pathology can be found in the hindfoot, midfoot, forefoot or a combination.

Figure 1: A cavovarus foot
Biomechanical consequences
- The weightbearing area of the sole of the foot is reduced
- The subtalar joint axis is more vertical
- The talar head is externally rotated over the anterior process of the calcaneum
- The subtalar and Chopart joints are more rigid
- The foot is generally “stiffer” than normal
- The ability of the foot to absorb impact is reduced
Aetiology
- All forms of cavovarus foot essentially result from muscle imbalance
- Can be divided into 2 main groups:
Neuromuscular
- 50% of all detectable lesions are a variant of Charcot Marie Tooth disease
- in unilateral, progressive cavus foot, consider spinal cord tumour
Non-neuromuscular
- idiopathic
- the 'subtle cavus foot'
- most are due to a plantar flexed 1st ray (?peroneus longus overactivity?)
- traumatic (compartment syndrome, burns, fracture malunion)
- undertreated talipes equinovarus
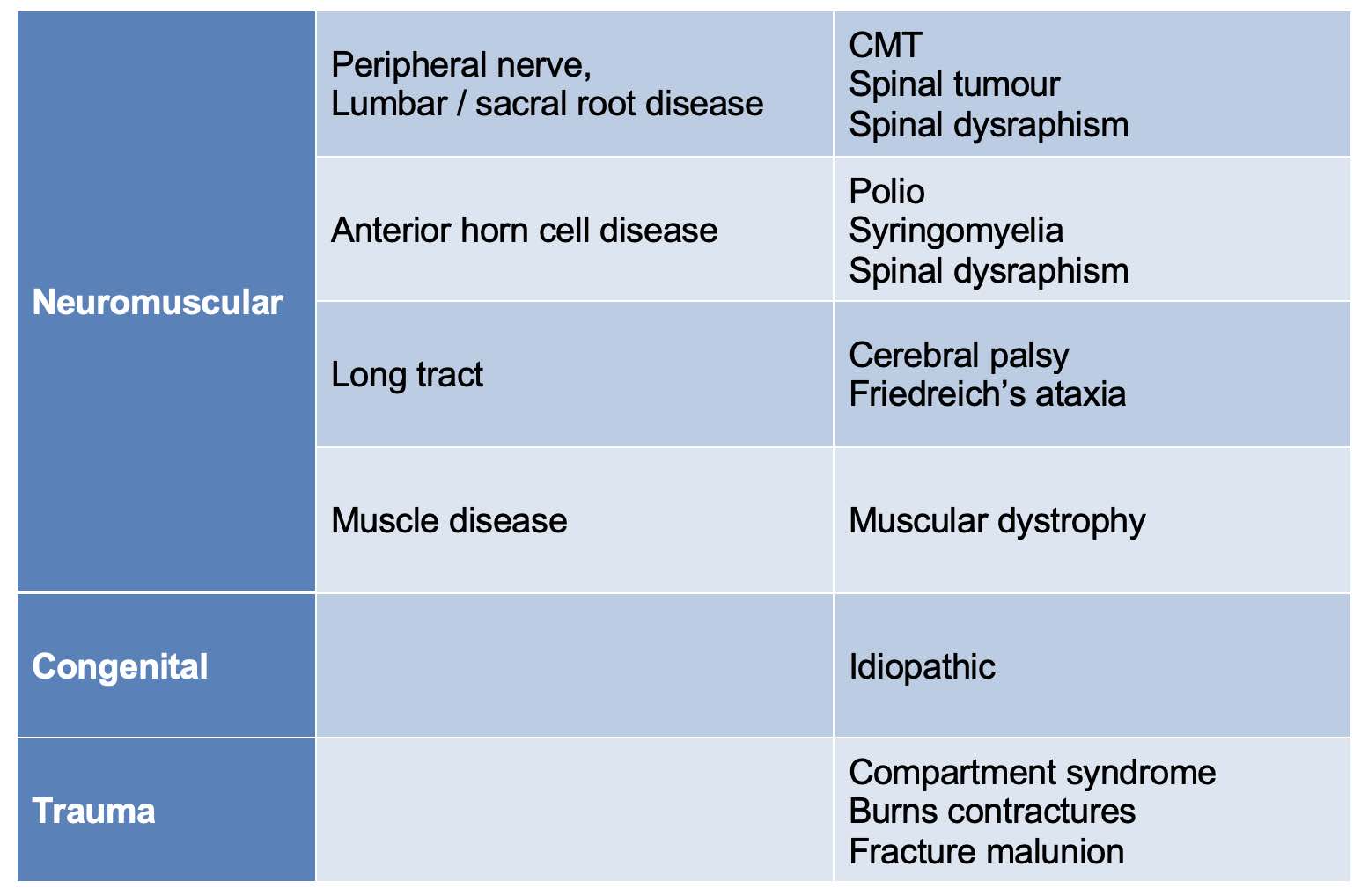
Table1: Classification of cavus foot aetiology
Charcot Marie Tooth Disease
- In 1886:
- Jean Martin Charcot and Pierre Marie (France) were physicians who described the condition
- Howard Henry Tooth (UK) described the peripheral nerve pathology
- 50% of all detectable lesions causing a cavovarus foot
- Essentially a myelin sheath disorder; various types and inheritance, often with varying levels of penetration:
- Most common (50%): autosomal dominant / sporadic
- Next most common: autosomal dominant
- X linked: 10-20% of cases
- Rarest: autosomal recessive
Deformity vs muscle imbalance
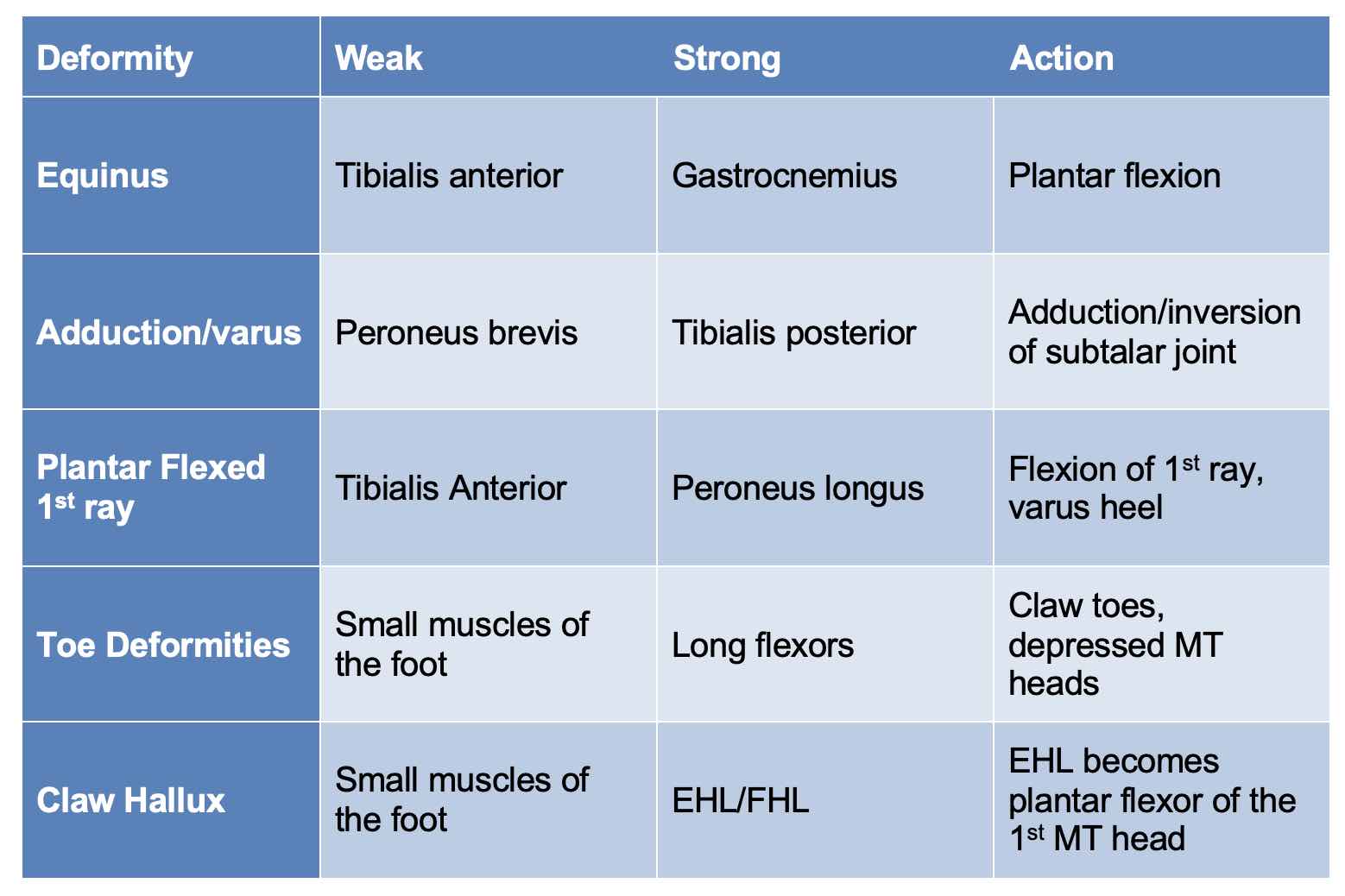
Table 2: Deforming forces in a cavus foot
History
- Pain and symptoms
- Family history
- Progression
- Unilateral vs bilateral
- Shoes
- Treatment so far
Examination
Remember to do a full neurological exam; there is almost always a neurological condition as a cause (50% will be CMT).
Look at the lumbar spine:
- scars
- hair at the base of the spine
- scoliosis
In the unstable ankle, always look carefully for a (subtle) cavo varus deformity
The Coleman Block Test

Figure 2a: Markedly varus right heel, adducted forefoot
Figure 2b: The outer border of the affected foot is placed on a 2cm board allowing the first ray to drop down; In this case, the heel corrects to neutral / slight valgus with apparent correction of the forefoot adductus.

Figure 3: Side view showing the first ray dropping down to the floor, effectively removing a deforming force
A positive Coleman block test (Fig 2) confirms that:
a) the subtalar joint is flexible and
b) at least part of the deformity is driven by a flexed first ray ("forefoot-driven"); this will need to be addressed to correct the deformity
Management
“The goal - as in any foot surgery - is a plantigrade, comfortable foot”
Conservative treatment
- Orthoses (mostly accomoodative due to relative stiffness):
- accommodative insoles (offloads bony prominences - MT heads, base of 5th MT), heel raise for equinus
- corrective (e.g. heel wedge/tilt)
- AFOs
- Physiotherapy / calf stretching
Surgical Treatment
Decisions:
- Where is the deformity?
- Hindfoot / midfoot / forefoot or a combination?
- Is the deformity rigid or flexible?
- Can I balance the soft tissues or do I have to perform bony procedures?
- Severity of the deformity
Soft tissue options:
- Gastrocnemius / Achilles lengthening
- Tibials posterior tendon transfer (last muscle to fail in CMT)
- Peroneus longus to brevis tendon transfer (converts PL from a flexor of the first ray to a pure evertor of the foot)
- EHL transfer / tenodesis (Jones procedure combined with a fusion of the IPJ for claw hallux; also elevates the 1st ray)
- Flexor-extensor tendon transfer (FETT) procedure
- Plantar fascia release (Steindler release)
Bony options:
- Lateral heel shift / Dwyer osteotomy
- In polio, can do proximal translation of calcaneum (Samilson)
- Extension osteotomy of the 1st ray
- Midfoot osteotomy
- Triple fusion
Surgery is based on careful preoperative assessment of the whole condition. It is best regarded as a palette of procedures applied to the individual patient's deformity.
One size does not fit all!

FIgure 4: Radiograph of a cavovarus foot treated with calcaneal osteotomy, extension osteotomy of the first ray and tibialis posterior tendon transfer. Note - despite excellent correction, the patient required subsequent exostectomy of calcaneal plantar prominence.
References
Seaman TJ, Ball TA. Pes Cavus. 2023 Aug 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan PMID: 32310476
Abbasian A, Pomeroy G. The idiopathic cavus foot-not so subtle after all. Foot Ankle Clin. 2013 Dec;18(4):629-42
Aminian A, Sangeorzan BJ. The anatomy of cavus foot deformity: Foot Ankle Clin. 2008 13: 191-198 2008
Ward CM, Dolan LA, Bennett DL, et al.: Long term results of reconstruction for treatment of flexible cavovarus feet in Charcot-Marie Tooth disease. J Bone Joint Surg Am. 2008 90:2631-2642 2008
Maskill MP, Maskill JD, Pomeroy GC. Surgical management and treatment algorithm for the subtle cavo varus foot. Foot Ankle Int. 2010;31(12): 1057-63
Manoli A 2nd, Graham B. The subtle cavus foot, "the underpronator". Foot Ankle Int. 2005 Mar;26(3):256-63. doi: 10.1177/107110070502600313. PMID: 15766431
Samilson RL. Crescentic osteotomy os cslcis for calcaneovarus feet. Bateman JE Foot science. 1976 WB Saunders Philadelphia 18
Brewerton DA, Sandifer PH, Sweetnam DR. “Idiopathic” pes cavus: an investigation into its aeitiology. Br Med J. 2: 659-661 1963