Part 5: Fractures
- Plain radiographs are the mainstay of trauma imaging
- At least two radiographic views at 90˚ to each other must be taken of any suspected injury
- Ideally 3 views for foot trauma - AP, oblique and lateral
- Weight-bearing comparison views can be helpful
Salter-Harris fracture
Involves the physis of an immature skeleton.
Classification can be remembered using the mnemonic SALTR:
- Slip of the physis
- Above the physis
- Lower than the physis
- Through the physis
- Rammed physis
Tillaux fracture
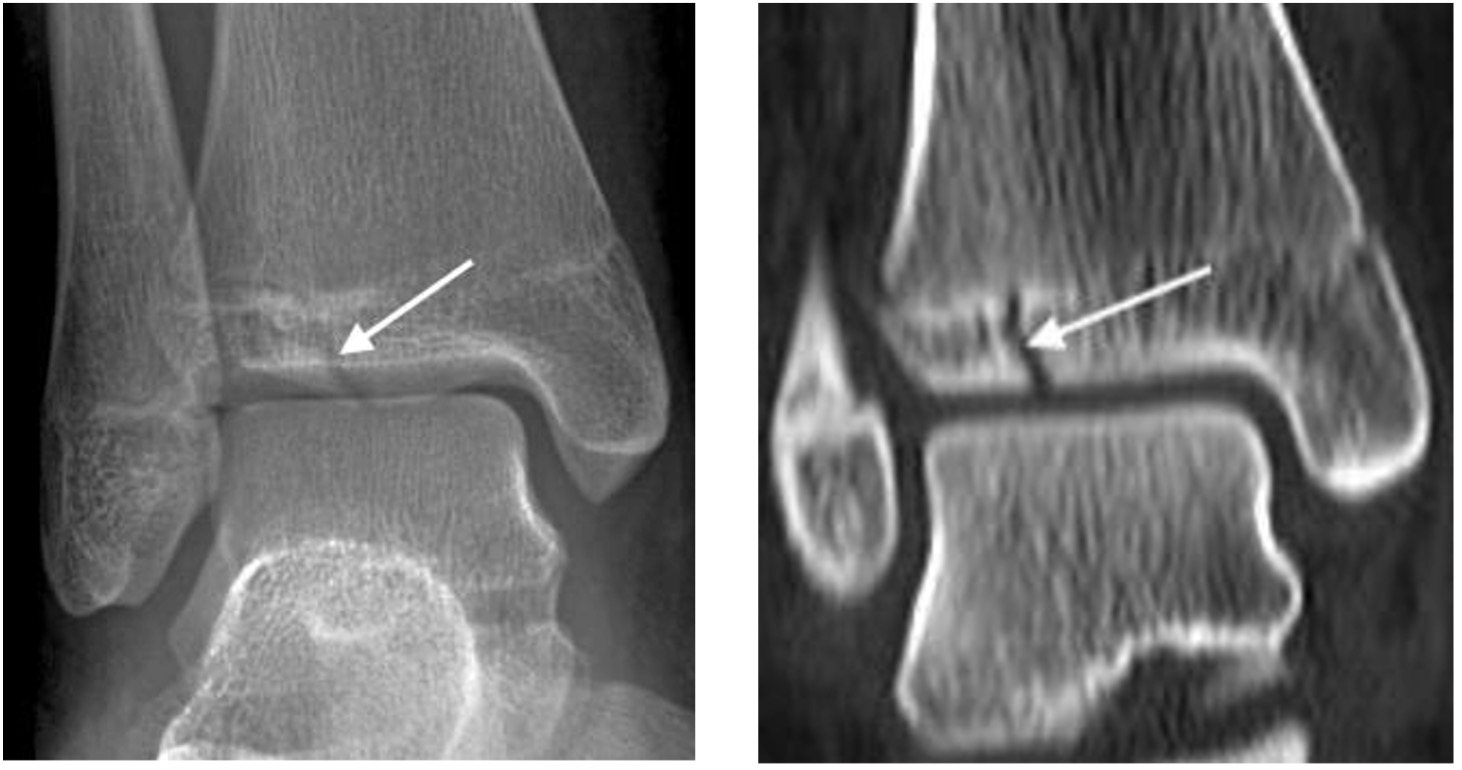
Salter-Harris type 3 fracture through the anterolateral distal tibial epiphysis.
Variable displacement. Occurs in older children and adolescents when the medial distal tibial growth plate has started to fuse.
Triplanar fracture
- Salter-Harris type 4 fracture through the lateral distal tibia with sagittal, axial and coronal plane components
- Comprises a vertical fracture through the epiphysis, horizontal fracture through the physis and oblique fracture through the metaphysis
*awaiting image upload*
Triplanar fracture extending through the distal tibial epiphysis, physis and metaphysis (arrows)
Danis-Weber ankle fracture classification
- For description of lateral malleolar (distal fibula) fractures
- Relates to the level of the fracture in relation to the ankle joint
Weber A

- Below level of the talar dome
- Usually transverse (pull-off)
- Tibiofibular syndesmosis intact
- Deltoid ligament intact
- Medial malleolus occasionally fractured (push-off)
- Usually stable if medial malleolus intact
Weber B

- At level of the talar dome; may extend proximally
- Usually spiral
- Syndesmosis usually intact, but widening of the distal tibiofibular joint indicates syndesmotic injury
- Medial malleolus may be fractured or
- Deltoid ligament may be torn
- Variable stability; depends on status of medial structures and syndesmosis
Sub-classification:
B1: isolated
B2: associated with a medial lesion (# or ligament)
B3: associated with a medial lesion and posterior tibial fracture
Weber Type C

- Above level of the syndesmosis
- Syndesmosis disruption with widening of distal tibiofibular articulation
- Medial malleolar fracture or deltoid ligament injury
- Fracture may arise as proximally as the fibular neck
NB: If a medial malleolar fracture and/or widening of the mortise joint is noted, proximal radiographs should be performed to rule out a proximal fibular (Maisonneuve) fracture.
Pilon fracture

- Distal tibial fracture with intra- articular extension
- Usually compression (axial-loading) injury
- Often fall from height
- Check for other injuries: talar, calcaneal or spinal fracture
Talar neck fracture
- Impaction of talus on tibia during forced ankle dorsiflexion
- May lead to disrupted blood supply to the talar body with subsequent avascular necrosis
- The ‘Hawkin's sign' describes subchondral lucency of the talar dome 6-8 weeks after a talar neck fracture; indicates sufficient vascularity in the talus
- Absence of the Hawkins sign, seen as subchondral sclerosis may indicate disruption to the blood supply of the talar dome and underlying AVN

Hawkin’s sign with subchondral lucency of the talar dome (arrows)
Calcaneal fracture
Usually from a fall from height
Extra-articular: 25-30%
- Anterior calcaneal process fracture, calcaneal tuberosity avulsion, extra-articular body fracture, sustentaculum
Intra-articular: 70 – 75%
- Usually comminuted
- ‘Double density’ sign due to impacted fracture, subtalar incongruity and separation of sustentaculum
- Decreased Bohler’s angle <20°
- Increased Gissane angle >145°
- Shear fracture in sagittal plane splits calcaneus into anteromedial (sustentacular) and posterolateral (tuberosity) fragments.
- Compression fracture in coronal plane with anterior limb running through critical angle of Gissane and posterior limb extending either horizontally in axial plane toward the tuberosity in tongue type fracture or more vertically, behind the posterior facet in joint depression type fracture.
- Look for lateral malleolar ‘fleck’ sign which raises likelihood of peroneal tendon instability.

Calcaneal fracture: tongue type Calcaneal fracture: joint depression type
Chopart fracture
- Fracture-dislocation through the midtarsal joint (calcaneocuboid and talonavicular)
Lisfranc fracture
- Fracture-dislocation of the tarsometatarsal joints
- Key to normal alignment:
- medial border of the 2nd MT should line up with the medial border of the intermediate cuneiform on the AP view
- medial margin of the 3rd MT should line up with the medial margin of the lateral cuneiform on the oblique view
- May be missed if subluxation is minimal
- Gap > 2mm between bases of 1st and 2nd MTs is abnormal
- ‘Fleck sign’ indicates small avulsion fragment, from lateral edge medial cuneiform or medial 2nd MT base

Lisfranc fracture with widening between 1st and 2nd MT bases, malalignment of the 2nd metatarsal (2MT) and intermediate cuneiform (IC). Fleck sign (arrow) indicating small avulsion from 2nd MT base
Fifth metatarsal base fractures
Avulsion fracture
- Caused by pull off peroneus brevis tendon
- Differentiate from normal unfused apophysis:
- the apophysis lies parallel to the long axis of the MT
- a fracture line lies transverse to the long axis of the MT
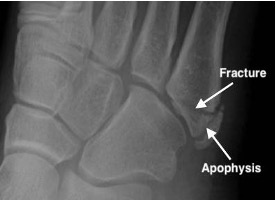
Avulsion fracture base 5th metatarsal and normal apophysis
Jones fracture

- Extra-articular transverse fracture at the metadiaphyseal junction of the fifth metatarsal
- Higher chance of non-union due to watershed vascularity
Stress fracture

- Occurs as a result of repetitive stresses or overload on bone
- Recognised sites include:
- tibia and fibula in long distance runners
- calcaneum and metatarsals secondary to walking (“March fracture”) and prolonged standing
- Seen as a linear band of sclerosis with periostitis
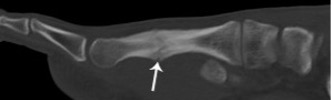
3rd metatarsal stress fracture with periostitis (arrowheads)