Amputations around the foot and ankle
Introduction
- Various indications:
- diabetic foot ulcer responsible for 75-85% of all lower limb amputations
- trauma
- infection
- tumour
- congenital deformity
- Reserved for patients where the foot is unsalvageable once all devitalised tissue has been removed
- May be performed as primary procedure, or as part of a staged approach after initial debridement
- Post-operatively, ALL patients should have input from the orthotic / prosthetic team to ensure safe loading of the remaining foot
Principles
- Preservation of limb where possible
- The more proximal the amputation, the greater the impact on the function of the remaining limb and the greater the energy requirement in gait
- Consider more proximal amputation if provides better functional result
- Control of infection with pre-operative antibiotics and local antibiotic preparations
- Ensure good vascularity to stump; early involvement of vascular team; predictors of adequate perfusion: ABPI >0.5, toe pressure >30mmHg, oxygen perfusion pressure >37mmHg
- Consider patient factors e.g medical co-morbidities, smoking, premorbid function
- Good nutritional status; indicators of poor wound healing: albumin <3.5g/dl and lymphocyte count <1500/ml
- Meticulous technique: no tourniquet, strict haemostasis
- Glucose control to maintain low HbA1c in diabetics essential
- Avoidance of dehydration increases tissue perfusion
- Patients with poor renal function generally take longer to heal
Currently, the most important types of amputation to be aware of are transmetatarsal and Symes amputations. Boyd has a role to play in paediatrics. Lisfranc, Chopart and Pirogoff are important to be aware of but are more of historical importance.
Level of amputation
- Determined by level of bony involvement and amount of soft tissue available after debridement to allow closure of wounds and healing with stable soft tissue envelope
- Can be partially determined pre-operatively with imaging (usually MRI), but final decision needs to be made after debridement back to healthy, bleeding tissue
Toe / partial ray amputation
- Common in diabetics
- Minimal amount of foot removed, so least impact on gait
- Chance of further amputation (ray / transmetatarsal / below knee) of around 25%
- If the amputation involves the base of the 5th metatarsal, then must consider reinsertion / transfer of the peroneus brevis tendon to prevent imbalance
Transmetatarsal
- Less functional than an amputation that preserves some of the medial column (1st or 2nd ray)
- Common in both peripheral vascular and diabetic patients; in these patients, 75% will be able to walk independently with an aid once healed
- 8% mortality rate at 1 year highlights the end organ damage that is occurring in these patients
- Around 30% of patients will require a further amputation in their lifetime
Indications
- Healthy tissue proximal half of metatarsals
- Non-viable tissue secondary to (in decreasing frequency): diabetic foot, vascular insufficiency, trauma (Others: infection, osteomyelitis, neoplasms)
Rationale
- Tibialis anterior preserved hence counteracts equinus contracture
- Preserves as much foot length as possible so can wear modified shoe rather than prosthesis; in non-ambulant patients with poor healing potential, consider more proximal resection
Surgical technique
- Transverse dorsal incision at level of mid-metatarsal shafts, dissect through to subcutaneous tissue
- Terminal branches of cutaneous peroneal nerves identified, tensioned and transected sharply
- Plantarflex forefoot to stretch extensor tendons at level of dorsal incision and divide
- Metatarsals osteotomised with bevelled oblique angulation at 20 degrees distal dorsal to plantar proximal; maintain metatarsal cascade: cut each MT 2mm shorter than the previous
- Fashion a thick plantar flap by extending incision 45 degrees across medial and lateral foot distally to level of metatarsal heads then extend incision transversely across just proximal to metatarsal heads
- Dorsiflex the remaining forefoot to identify the flexor tendons and cut these under tension
- Terminal branches of medial plantar nerve, nerve to 1st ray and medial plantar artery are identified and ligated
- Myodese the plantar flap onto the residual metatarsal heads
- Skin closure with nylon
Complications
- Delayed primary healing
- Failed primary healing
- Plantar ulceration
- Stump ulceration / blistering
Post amputation prosthesis
- Toe filler (Figure 1)
- Extended foot plate
- Rigid rocker-bottom sole


Figure 1: Silicone foot protector in combination with a shoe filler to accommodate missing forefoot
Lisfranc (tarso-metatarsal joint level)
- Through Lisfranc or Chopart joints
- Fell out of favour due to equinus contracture, difficulty balancing tendons and re-ulceration
- When combined with gastro-soleus lengthening and re-implantation of tendons (esp tibialis anterior and peronei), better outcomes and function achievable
- Again, high re-amputation rate of around 30%
- A well-designed and fitted prosthesis will improve functional outcome
Indications
- Diseased tissue extending to the proximal metatarsals but not breaching beyond the tarso-metatarsal joints.
Rationale
- Can mitigate against equinovarus deformity to preserve insertion of tibialis anterior at medial cuneiform and peroneus brevis tendon at base of 5th metatarsal (Sanders modification); traditional Lisfranc amputation failed to do this
Surgical technique
- Base of 2nd metatarsal should be preserved to preserve proximal transverse arch
- Transverse incision at proximal 1/3 of metatarsals; cutaneous branches of peroneal nerve identified and sharply transected; terminal branch of dorsalis pedis artery ligated
- Flex forefoot to stretch extensor tendons and divide
- Disarticulate the Lisfranc joint at the tarso-metatarsal level; try to mitigate against equinovarus deformity by preserving insertions of tibialis anterior and peroneus brevis
- Incision extends plantarwards at 45 degrees to the dorsal incision to allow for a soft tissue plantar flap
- Medial and lateral plantar nerves and vessels are ligated; the plantar flap is then myodesed to the tarsal bone stump
Complications
- Equinovarus deformity if failed tendon preservation
- Skin and wound breakdown
Post amputation prosthesis
- Ankle-foot orthoses with a built in moulded insole; carbon-fibre plate with posterior opening door
- As leg length is maintained on the amputated side, the addition of a prosthesis may lead to lengthening hence use of heel raise on contra-lateral side may be required
Chopart (transverse tarsal joint level - through calcaneocuboid and talonavicular joints)
Indications
- Diseased tissue must not extend proximal to midfoot level
Rationale
- Through Chopart’s joint (talonavicular and calcaneocuboid)
- Easier to perform than Symes; less limb shortening; preserves tough weight-bearing skin of heel
- Poor choice for active patients
Surgical technique
- Fish-mouth incision at level of transtarsal joints; extend flaps in dorsal and plantar direction to ensure coverage; tension sensory nerves, cut flush, let retract
- Identify tibialis anterior and peroneus brevis, divide and prepare for tendon transfer
- Disarticulate the calcaneocuboid and talonavicular joints after releasing the dorsal and plantar ligaments
- Tibialis anterior tendon transferred to neck of talus; peroneus brevis transferred to anterior process of calcaneum
- Approximate fascial layers plantar and dorsally and close skin in tension-free manner
Complications
- Equinus deformity - may be addressed with Achilles tenotomy and position of ankle in dorsiflexion for 6 weeks; ankle arthrodesis if this fails
- Stump pain
- Skin and wound breakdown
Post amputation prosthesis
- Ankle-foot orthoses with a built-in moulded insole; carbon-fibre plate with posterior opening door (Figure 2)
- As leg length is maintained on amputated side, the addition of a prosthesis may lead to lengthening; hence a heel raise on contra-lateral side may be required

Figure 2: Carbon-fibre AFO with posterior opening door
Boyd
- Boyd amputation involves fusion of calcaneal posterior facet to the distal tibia (cf Pirogoff below)
- MUST have patent posterior tibial artery for calcaneum and heel pad skin to survive
- Maintain length and provide a stump on which one can walk short distances
Indications
- Role in paediatrics; amputation strategy in treatment of fibular hemimelia
- Louie(2010): Boyd preferable to Symes in type 2 fibular hemimelia (complete fibular absence); less pain and greater satisfaction
- Heel pad less than optimal sensibility or where distal tibia badly damaged or atrophic
Rationale
- Allows less limb shortening; important in paediatric setting where Symes will result in limb length similar to trans-tibial amputation at skeletal maturity
- Produces an end-bearing stump with no migration of heel pad
Surgical technique
- Fish-mouth incision; dorsal incision over tibio-talar joint; plantar incision at distal extent of heel fat pad; extend plantar incision down to bone
- Plantarflex foot, transect dorsal nerves and extensor tendons
- Expose tibiotalar joint by releasing anterior capsule; divide deltoid and talofibular ligaments; bone hook on talar dome to expose posterior capsule – this is divided while protecting neurovascular bundle which lies medial to FHL
- Divide talocalcaneal ligaments and remove talus; midfoot and forefoot are then disarticulated and removed
- Oscillating saw is used to remove anterior process of calcaneum and superior articular surface of calcaneum using a horizontal cut
- The distal tibia is then cut similar to Symes cut; cancellous bone ends of tibia and calcaneum are reduced and held together with a retrograde K-wire across calcaneo-tibial ends; screw fixation of the calcaneum to tibia can be performed or can be held with temporary Steinmann pin for 6 weeks until fusion
Complications
- Symptomatic non-union
- Tibio-calcaneal mal-union; if calcaneum fixed in varus can lead to roll over lateral foot in midstance; difficulty with pain and prosthetic fitting may necessitate revision to Symes
- Excess limb length
- Infection, wound dehiscence
- Steinmann pin migration
Post amputation prosthesis
- Initially, space limitation is a problem as with Pirogoff amputation; however, as the child grows, shortage increases compared to contralateral side such that standardised carbon-fibre prosthesis can be used at skeletal maturity
Pirogoff
Indications
- If patient is low demand and will not use a prosthesis
- (Modified) Pirogoff amputation involves excision of the anterior part of the calcanuem and fusion of the remnant to the distal tibia
Rationale
- Longer soft tissue flaps and less limb shortening compared to Symes
- No obvious advantage over Boyd and technically more challenging
- Requires calcaneo-tibial fixation and fusion
Surgical technique
- The approach for the Pirogoff amputation is similar to Boys, up to the point of calcaneal osteotomy
- Once the talus has been removed and the midfoot disarticulated, the calcaneum is first osteotomised vertically just behind the anterior facet of calcaneum allowing the distal ¼ of calcaneum to be removed
- A second oblique cut is made at 60 degrees to this cut aiming towards posterior border of upper end of calcaneum; this wedge of bone is then removed leaving the remaining calcaneum within the soft tissue flap
- The tibia is osteotomised as in Symes technique; the remaining calcaneum is reduced onto the tibia surface and held with K-wires in a crossed manner; partially-threaded cannulated screws can then be inserted to hold the position
- The anterior and posterior flaps are then repaired
Complications
- Symptomatic non-union
- Infection, wound dehiscence
- Stump breakdown
- Stump hyperkeratosis
Post amputation prosthesis
- Elephant boot (seldom used): simple leather pouch that encases the residual limb and fastens above the malleoli with a drawstring; may have a role in the developing world where prosthetic care not available
- Short shoe: interior custom-moulded foot orthosis, steel shank and mini-rocker sole (Figure 3)

Figure 3: Scotchcast orthosis with short shoe and total contact insole
Syme
- Through-ankle amputation with removal of articular cartilage and malleoli; heel pad attached to the distal tibia
- Watch for heel pad migration and bony regrowth (particularly in the paediatric amputations for congenital abnormalities)
- Well tolerated in the paediatric population with 80% able to walk on the stump for short distance; most are able to participate in sporting activities
- Less well tolerated in adults – only 40% able to walk on the stump
Indications
- MUST have patent tibialis posterior artery to heel pad
- Diabetic neuropathy is a relative contraindication due to lack of protective sensation
- Higher demand / more athletic individuals: increased shortening will allow for carbon-fibre prosthesis
- Can ambulate short distances without a prosthesis (e.g. toilet at night)
Rationale
- Space available for self-suspending prosthesis and artificial foot
- Heel pad is a normal weight-bearing surface, hence reduces chance of phantom limb discomfort
- Produces an end-weight-bearing stump
- Advantages over BKA include:
- Preservation of lower leg segment
- Greater quadriceps lever arm = more energy efficient
- 10% more energy required per extra step compared with 24% for BKA
- Minimal prosthetic training required
- Greater stride length
Surgical technique
- Mark out points 2cm anterior and inferior to medial and lateral malleoli
- Aim not to encroach on the heel fat pad
- Dorsal incision connecting two points extended over dome of talus
- Plantar incision down to calcaneum from these points
- Ligate dorsalis pedis artery and resect tib ant and dorsiflexor tendons
- Release ligamentous attachments to talus
- Enucleation of the talus and calcaneum from the soft tissues (can use an external fixator pin into talus to act as a joy-stick for retraction)
- Preserve medial neurovascular bundle to preserve blood supply to stump
- Protect subcutaneous attachment of Achilles; subperiosteal dissection of calcaneus
- Cut malleoli flush with plafond using an oscillating saw
- Heel pad translates directly proximally, thereby creating dog ears and ensuring mid heel pad is in the middle of the resected tibial surface
- Fibrin spray for 2mins prior to using 2mm k-wires to hold the flap in place and avoid translation
- Plantar fascia sutured back to deep fascia anteriorly prior to skin closure
- Consider a LA catheter, drain and incisional VAC
- NWB for 6 weeks, after which K-wires are removed


Figure 4: Left: incision marking for Symes amputation, Right: soft tissue dissection during Symes

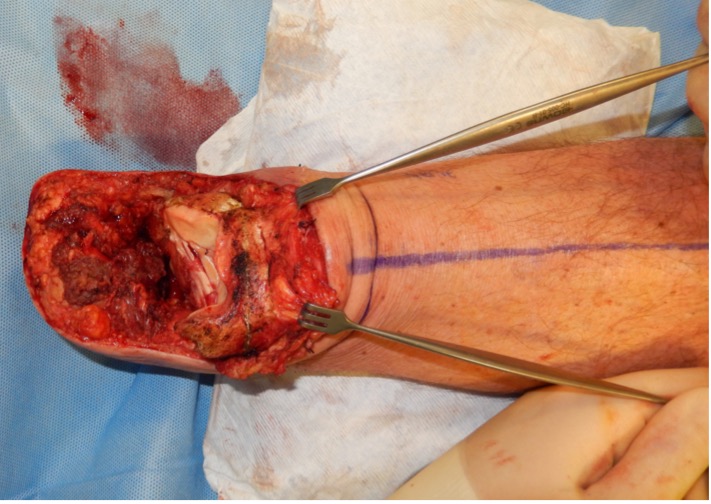
Figure 5: Left: ankle joint disarticulation during Symes, Right: following enucleation of the talus and calcaneum, the heel pad flap is preserved; the malleoli can still be seen and next step would be cutting the malleoli flush with the plafond

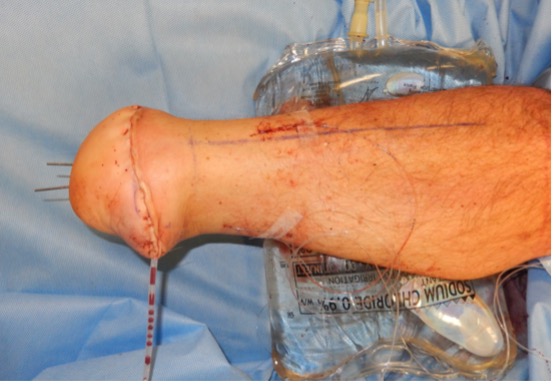
Figure 6: Left: the flap is fashioned to cover the stump, Right: the flap is held with multiple k-wires, a drain is inserted as well as a local anaesthetic catheter


Figure 7: Left: healthy stump after k-wire removal at 6 weeks, Right: the stump has healed well
Complications
- Early failure: heel pad dysvascular necrosis
- Heel pad migration
- Distal bony prominence
- Hypermobility of stump
- Neuroma formation
- Heel pain
- Dog ears medial / lateral
Post amputation prosthesis
- Sophisticated carbon-fibre foot ankle prosthesis

Figure 8: AFO with total contact insole and accommodative footwear
MCQs
A Symes amputation is advantageous over a below knee amputation in all of these cases EXCEPT?
- minimal prosthetic training required
- reduced stride length
- greater energy efficiency
- fewer stump problems
Which one of the following factors is an absolute contraindication to Symes amputation?
- lack of a viable heel pad
- high demand individuals
- ABPI =0.5
- smoking
Midfoot amputations such as the Chopart or Lisfranc amputation are commonly associated with which complication?
- equino-varus
- equino-valgus
- infection
- plano-valgus
- metatarsus adductus
Which of the following statements is NOT true of a trans-metatarsal amputation?
- a transmetatarsal amputation is beneficial as it can avoid use of prosthesis and retains limb length
- a transmetatarsal amputation can be beneficial as it avoids an equinovarus deformity
- a transmetatarsal amputation should be considered when diseased tissue involves the proximal 1/3 of the metatarsals
- a more proximal amputation should be considered if there are any concerns regarding wound healing
Which of the following amputations has been described in the paediatric setting, particularly in the maintenance of limb length before skeletal maturity?
- Symes
- Pirogoff
- Boyd
- Chopart
- Lisfranc
Which one of the following amputations involves a talo-calcaneal fusion?
- Boyd
- Chopart
- Symes
- Lisfranc
References
Andronic O et al. (2019). Modifications of the Pirogoff Amputation Technique in Adults: A Retrospective Analysis of 123 Cases.Journal of Orthopaedics, 18, 5-12
Braaksma R et al. (2018). Syme Amputation: A Systematic Review. Foot & Ankle International, 39(3), 284–291
Borkosky SL & Roukis TS. (2012). Incidence of re-amputation following partial first ray amputation associated with diabetes mellitus and peripheral sensory neuropathy: a systematic review. Diabetic Foot & Ankle, 3(1), 12169
Canale, S. and Campbell, W. (2000). Campbell's operative orthopaedics. St. Louis, MO: MD Consult LLC
Coughlin, M., Saltzman, C., Anderson, R. and Mann, R. (2014). Mann's surgery of the foot and ankle. Philadelphia: Saunders/Elsevier
Calder, P., Shaw, S., Roberts, A., Tennant, S., Sedki, I., Hanspal, R. and Eastwood, D. (2017). A comparison of functional outcome between amputation and extension prosthesis in the treatment of congenital absence of the fibula with severe limb deformity. Journal of Children's Orthopaedics, 11(4), pp.318-325
Louie B, Lerman J, Walker J, Bagley A (2010). Syme vs Boyd Amputation for fibular deficiency: A Two Center Functional Assessment Study. Conference: 2010 American Academy of Pediatrics National Conference and Exhibition
Nather A & Lin Wong K. (2013). Distal amputations for the diabetic foot. Diabetic Foot & Ankle, 4(1), 21288
Janisse, D. and Janisse, E. (2010). Shoes, Orthoses, and Prostheses for Partial Foot Amputation and Diabetic Foot Infection. Foot and Ankle Clinics, 15(3), pp.509-523
Philbin, T., Leyes, M., Sferra, J. and Donley, B. (2001). Orthotic and prosthetic devices in partial foot amputations. Foot and Ankle Clinics, 6(2), pp.215-228
Thorud JC et al. (2016). Reoperation and Reamputation After Transmetatarsal Amputation: A Systematic Review and Meta-Analysis. The Journal of Foot and Ankle Surgery, 55(5), 1007–1012