Part 9: Advanced Imaging
ULTRASOUND (US)
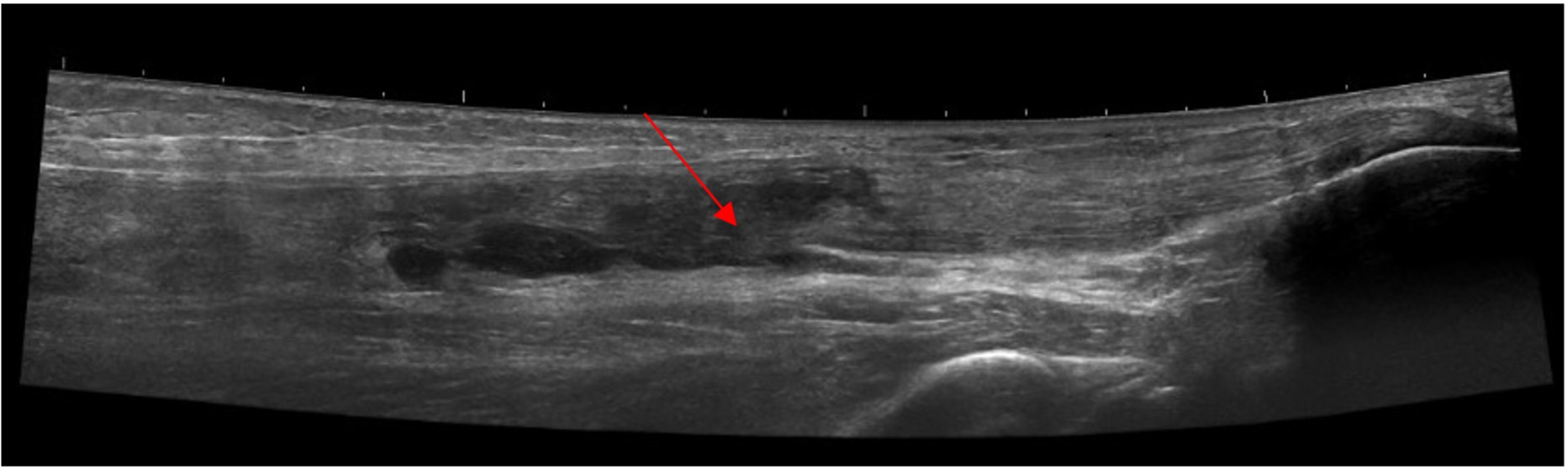
Ultrasound image of the Achilles tendon showing high-grade tear (red arrow) at the musculo-tendinous junction
Generation of US image
US examinations use reflections of sound waves to detect differences between soft tissue interfaces. When the sound waves encounter an interface between tissues of different density, reflection or refraction occurs.
Sound waves reflected back to the transducer are recorded and converted into images. US provides a real time image that may be obtained in any plane by simply rotating the transducer.
US appearances may be described in terms of echogenicity. Brighter areas such as cortical bone, calcium and fat are said to be echogenic or hyperechoic. Darker areas such as fibrous or scarred tissue are described as hypoechoic. Some tissues, such as fluid, produce no echoes; these are completely black referred to as anechoic.
Indications
US plays an important role if patients present with symptoms localised to a particular area of the foot. If symptoms are more diffuse, MRI may be more appropriate for more complete assessment and, in particular, to assess the bone and joint surfaces.
Tendon dysfunction – tendinopathy, tenosynovitis, tendon tears, tendon subluxation (value of dynamic scanning).
Specific soft tissue pathology – plantar fasciitis, Achilles tendinopathy / rupture, ligament injury, tarsal tunnel syndrome.
Soft tissue masses or collections (including Morton’s neuroma) – one of the most useful features of US is the ability to differentiate solid from cystic lesions. Although US may not be able to confirm a specific diagnosis, a purely cystic lesion can be assumed to be benign. An extension of ultrasound is Doppler imaging, which can detect and measure blood flow and this has an important role in assessing the vascularity of mass lesions.
Joints – joint effusion (seen as compressible black anechoic fluid) can be differentiated from synovial hypertrophy which has a more echogenic appearance. In active synovitis, increased synovial blood flow is demonstrated with Doppler imaging.
US-guided procedures – aspirations, injections, biopsies.
Limitations
- US images are transient and operator-dependent
- Bones and joint surfaces are not well visualised, especially the talar dome and subtalar joint
MAGNETIC RESONANCE (MR) IMAGING
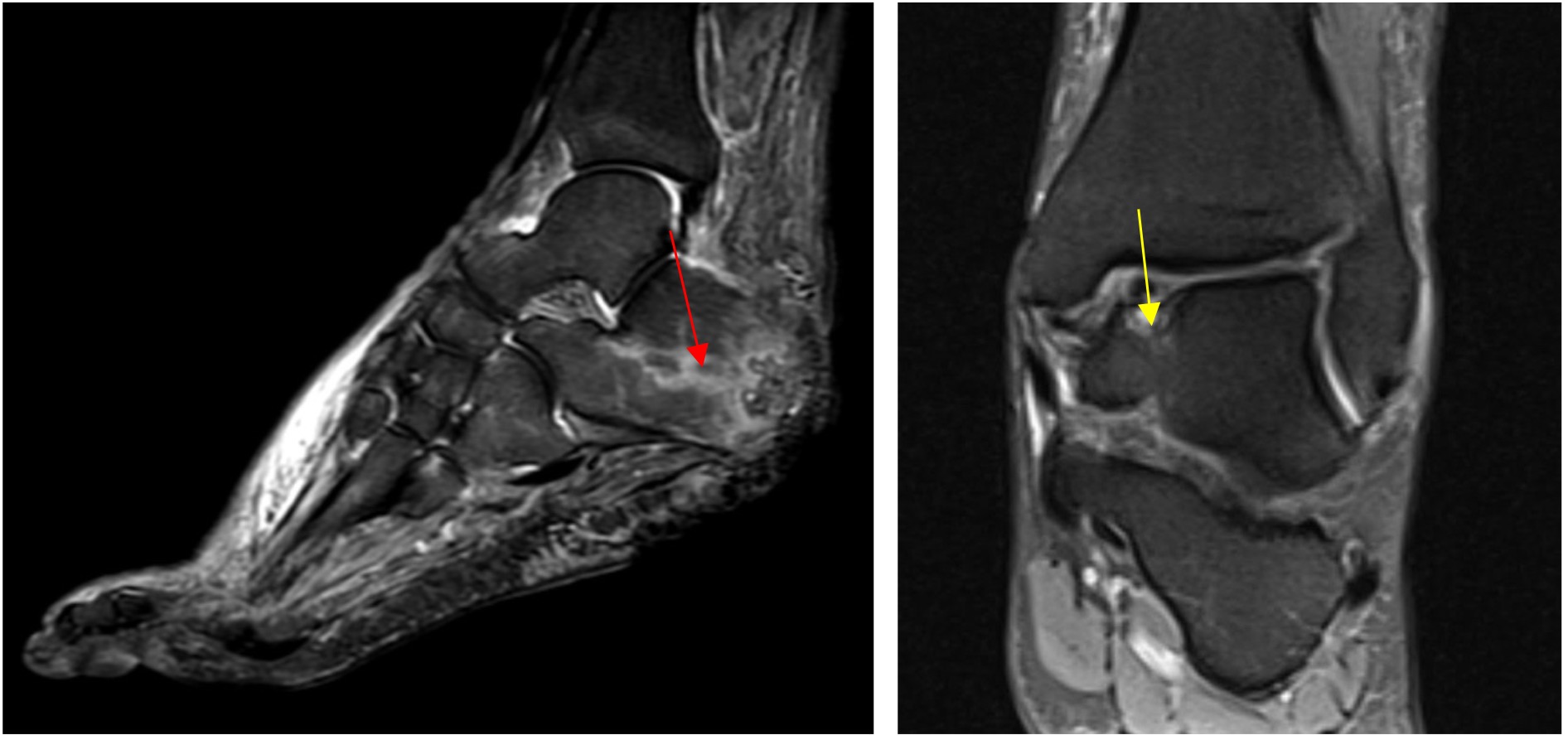
Left: Sagittal STIR sequence demonstrating calcaneal osteomyelitis (red arrow)
Right: Coronal PDFS sequence demonstrating talar dome osteochondral defect (yellow arrow)
Generation of MR image
MR images are produced by a combination of magnetic field and radiofrequency (RF) pulses. As the magnetic field is turned on, protons (hydrogen nuclei) in the tissues align in the axis of the powerful magnetic field. The RF pulses are then alternately switched on and off, allowing the protons to absorb and release energy.
In doing so, between RF pulses, the protons emit characteristic radio waves of their own. These signals can then be detected and converted by computers to build an image.
Tissues vary in their water content (and hence concentrations of hydrogen nuclei), depending on their nature and if pathology is present. The resultant signals therefore vary accordingly.
MR appearances are described in terms of signal intensity which refers to the strength of the signal that a tissue returns. A bright (whiter) area in an image is said to demonstrate high signal intensity, whereas a darker area is said to demonstrate low signal intensity.
Detailed high-resolution images of soft tissue and bone marrow are generated as thin ‘slices’ through the body part which can be obtained in sagittal, coronal and axial planes using different imaging sequences.
Standard MR sequences used in foot & ankle imaging
An MR sequence is a particular set of RF pulses used to achieve the desired image.
- T1 sequence provides good anatomical detail; fat returns high signal on T1 thus useful for detecting pathology in fat-containing structures such as subcutaneous tissues, sinus tarsi, bone marrow and to confirm osseous coalition.
- T2 sequence provides good contrast for evaluation of pathologic processes, with fluid and oedema seen as high signal. (Reminder tip: fluid = H2O = T2)
- STIR (short time inversion recovery) or PDFS (proton density fat suppression) are T2W type sequences with fat suppression. These sequences are called fluid-sensitive sequences, providing a good overview with fluid/oedema readily seen as high signal.
Indications
Bone marrow – bone tumours, osteonecrosis, osteomyelitis, stress fractures, trabecular microfractures, coalitions.
Soft tissue – soft tissue tumours, sinus tarsi syndrome, plantar fasciitis, tendons, ligaments, nerves. MR offers no advantage in imaging tendons if expertise in MSK ultrasound is available. MR imaging of tendon disease is best reserved for patients in whom bony pathology is also being considered.
Bone and soft tissue tumours – tumour characteristics (intra-osseous and soft tissue extent, compartmental involvement, neurovascular involvement, intra-articular extension), post-operative follow up to assess for residual or recurrent tumour.
Joints – arthropathy, articular cartilage, osteochondral fractures, intra-articular osteocartilaginous bodies. Intra-articular structures may be better demonstrated with an intra-articular injection of contrast material, although this is seldom required since the advent of high resolution 3T MRI units.
Limitations
- Expensive and time-intensive.
- Claustrophobia, certain pacemakers and surgical clips are contra-indications.
- Although MR is sensitive in detecting abnormalities of bone marrow, further osseous detail is limited and MR is less helpful for assessing periosteal new bone formation, bone fragments and fractures.
- Metallic objects such as ferromagnetic surgical clips result in focal loss of signal with distortion of the image. Newer metal artifact suppression (MARS) software is helpful to limit metallic artifact.
COMPUTED TOMOGRAPHY (CT)

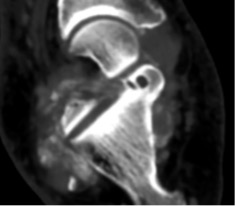
CT demonstrating subtalar joint non-union
Generation of CT image
The patient lies on the CT table and is moved slowly through the centre of a circular gantry containing a rotating X-ray generator and detectors. The narrow X-ray beams are absorbed or attenuated to various degrees depending on the density of the tissues being imaged.
The remaining unabsorbed or unattenuated X-rays pass through the tissue and are picked up by an array of detectors and processed by a computer. The CT software converts the beam attenuations of the tissue into an image which is digitised into a visual display.
Tissues with high attenuation (e.g. cortical bone) appear white; tissues with low attenuation (e.g. air) appears black; soft tissues with intermediate attenuation are variations of grey.
Usually 1.5 - 2mm contiguous axial sections are obtained through the foot and ankle which can be used to create multiplanar sagittal and coronal reformats as well as three-dimensional reconstructions.
Indications
The main use of CT is for the identification of bone-based pathology due to the excellent bone detail generated.
Fractures – fracture characterisation, intra-articular extension, fracture fragments, fracture union. Multiplanar reconstructions are helpful in pre-operative planning.
Bone lesions – lesion characterisation (matrix calcification, nidus of osteoid osteoma, stress fracture), intra-osseous extent, cortical breach, CT-guided biopsy or other (radiofrequency ablation, sclerotherapy).
Other specific bone and joint pathology – stress fractures, coalitions, osteochondral defects, loose ossific bodies.
Post-operative assessment – union of fusions, metalwork, alignment.
Limitations
- Ionising radiation
- Poor soft tissue contrast compared to MR
- Prostheses, rods, screws and other metal ware produce significant artefact
DUAL-ENERGY CT (DECT)
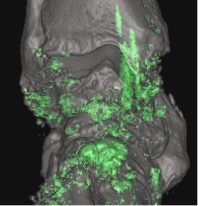
DECT demonstrates diffuse urate deposits in gouty arthritis (green areas)
Corresponding CT shows diffuse chondrocalcinosis
Generation of dual-energy CT image
CT technique that uses two separate x-ray photon energy spectra, allowing differentiation of tissues based on their attenuation properties at different energies.
Indications
Crystal arthropathies (gout, CPPD) – diagnosis confirmation/exclusion in subclinical disease, atypical presentations or gout-mimickers, problem-solving, monitoring treatment response by measuring disease burden.
Bone marrow oedema (trauma, oncology, inflammatory pathologies) – alternative in patients with contraindication to MR.
Optimise metal artefact reduction in cases of severe artefact.
Limitations
- Availability
- Higher dose of ionising radiation than standard CT
NUCLEAR MEDICINE (BONE SCAN)
Generation of bone scan image
Nuclear isotope scanning detects the distribution of a radiopharmaceutical (pharmaceutical labelled with radio-isotope) that is injected intravenously into the body. It relies on the fact that an inflamed or pathologically active area of the skeleton has increased blood flow and bone activity with increased radio-isotope uptake.
The radiopharmaceuticals most commonly used in bone scanning are phosphate markers, labelled with technetium-99. Following the injection, the patient is positioned under a gamma camera which detects the distribution of radioactivity in the body which is electronically displayed on a screen.
Indications
One advantage of skeletal scintigraphy over other imaging modalities is its ability to image the entire skeleton at once. However, with the increased availability of PET and SPECT scans, bone scans are becoming obsolete.
Bone tumours – particularly with multiple lesions such as metastases, multifocal tumours, skip lesions. Not so important now with whole body MRI. In most instances, bone scans cannot distinguish benign from malignant lesions because increased blood flow (with subsequent increased isotope deposition) and osteoblastic activity occurs in both conditions.
Active infection in chronic osteomyelitis – infected joint prosthesis (uptake > 12 months after joint replacement surgery is suspicious for prosthetic loosening or infection).
Limitations
For detecting pathology, scintigraphy is highly sensitive but not specific; it is often impossible to distinguish the various processes that result in increased isotope uptake.
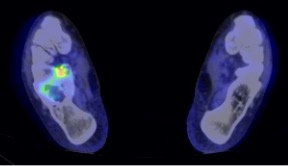
SPECT (Single photon emission computed tomography)
SPECT-CT demonstrating uptake in the posterior subtalar joint
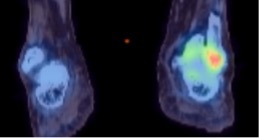
Different case showing uptake at the distal tibiofibular joint confirming main site of symptoms
Generation of SPECT image
SPECT is a three-dimensional nuclear medicine study involving radiopharmaceutical injection. The method of generating an image is similar to traditional planar nuclear imaging except that, instead of using a single gamma camera which produces planar 2D images, multiple gamma cameras rotate around the patient in a gantry, producing 3D images.
In simple words, SPECT is a 3D bone scan when used specifically for bones.
SPECT images can be combined with a CT scan to create a SPECT-CT, which provides both functional and anatomical information.
Indications
- To detect the source of foot or ankle pain (particularly useful in presence of implants when compared to MR).
- Localise the source of pain after joint fusion.
- Identify periprosthetic infection or loosening.
- Osteochondral defect, arthropathy, stress fracture, tarsal coalition, painful accessory bones, Achilles tendonitis, bursitis, plantar fasciitis, obscure pain.
Limitations
- Sensitive but not specific
- Availability
- Additional radiation exposure
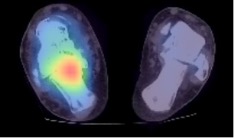
PET (Positron emission tomography)
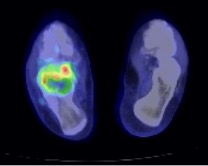
Pre-treatment PET-CT activity of giant cell tumour of the calcaneum showing marked peripheral FDG uptake
Post denosumab treatment PET-CT of the same lesion showing tumour response with reduced FDG uptake
Generation of PET image
A positron-emitting radiopharmaceutical is injected intravenously, and the scanner detects the quantity and pattern of accumulation in the body.
A PET scan can also be combined with CT, and in some centres with MR, to improve disease localisation.
F-18 Fluorodeoxyglucose (FDG)-PET scan localises areas of maximal glucose activity in the body. Tumour or infection are usually FDG-PET avid.
F-18 Sodium Fluoride-PET (NaF)-PET scan uses a radiotracer which localises areas of osteoblastic activity and is therefore more specific for bone pathologies.
Indications
- Evolving role in periprosthetic complications – sensitive but not specific for infection or loosening.
- Bone or soft tissue lesions – lack of PET activity is suggestive of benign pathology.
Limitations
- Sensitive but not specific
- Expensive, time-consuming with significant radiation dose
- High false positive rate due to inflammatory or post-surgical changes
- Availability
SUMMARY
- X-rays are ideal as first line imaging
- Consider ultrasound for localised pain, soft tissue lesions, tendon imaging and interventional procedures
- MR is useful for global foot and ankle pain, including bone marrow pathology and characterisation of tumours
- CT is good for assessment of fracture pattern, fusion and loose bodies
- DECT can be used as a problem-solving tool in gout-mimickers and in cases of severe metal artefact
- SPECT-CT is particularly helpful in the presence of implants to identify the source of post-operative pain
- PET-CT can be useful to characterise benign vs malignant lesions
- Both SPECT-CT and PET-CT are highly sensitive (but not specific) investigations for periprosthetic complications
- Ultrasound-guided aspiration/synovial biopsy or 111In-WBC scan are more specific for infection but are time-intensive and not readily available in all departments
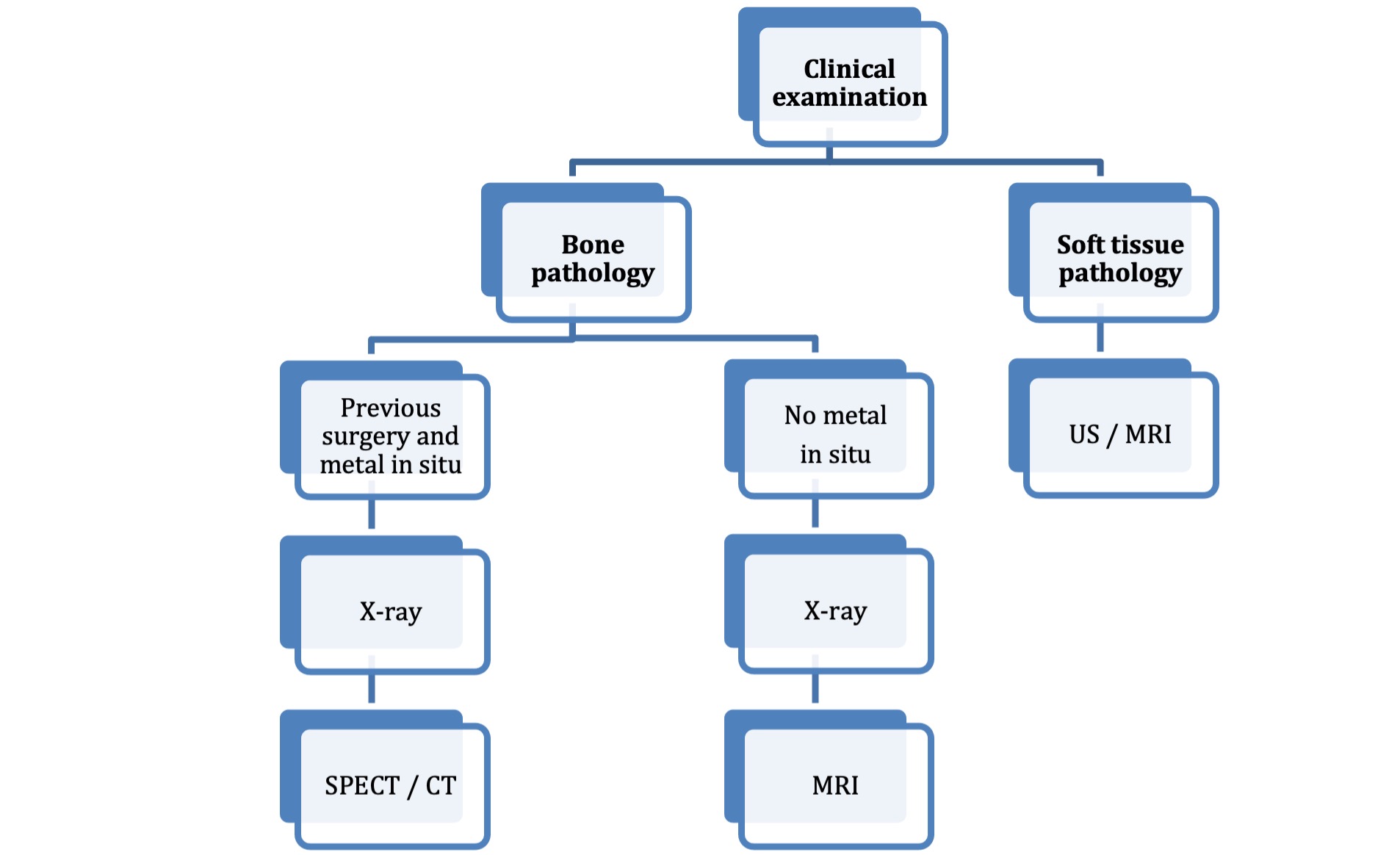
Diagnostic algorithm for imaging chronic foot pain
References
- Dual-Energy CT in Musculoskeletal Imaging: What is the role beyond gout? Rajiah P et al. Am J Roentgenol. 2019
- PET and SPECT in Osteomyelitis and Prosthetic Bone and Joint Infections: A Systematic Review. Van der Bruggen W et al. Semin Nucl Med. 2010
- SPECT/CT in Imaging Foot and Ankle Pathology – The Demise of Other Coregistration Techniques. Mohan HK et al. Semin Nucl Med. 2010