Part 8: Specific Joint and Soft Tissue Pathology
ASSESSMENT OF JOINTS
Rheumatoid arthritis
- Typically involves metatarso-phalangeal joints in a bilateral symmetrical fashion
- Early findings are soft tissue swelling, joint effusions and periarticular osteoporosis
- Progressive joint space narrowing and periarticular erosions as synovial pannus invades cartilage and bone
- Generalised osteoporosis and characteristic valgus deformities of the toes progressing to gross subluxation and dislocation in severe cases
- Midtarsal and hindfoot involvement is present in long-standing cases
- In juvenile disorders such as Still’s disease, there may be epiphyseal overgrowth and early fusion with delayed long bone growth and ‘spindling’ of the digits

Rheumatoid arthritis with symmetrical MTP joint loss, erosions and subluxation
Osteoarthritis
- Narrowing and irregularity of joint space
- Damaged cartilage may become calcified (chondrocalcinosis)
- Subarticular sclerosis with subchondral cysts Osteophytes
- Bone density usually maintained
- In late stages, the joint becomes partially or fully ankylosed and osteophytes may fracture, causing loose intra-articular bodies

Osteoarthritis of the 1st MTP joint with joint space narrowing, subarticular sclerosis and marginal osteophytes (arrows)
Gout
- Hyperuricaemia causes deposition of urate crystals
- First metatarso-phalangeal joint is commonly involved, termed a podagra
- Well-defined erosions with sclerotic borders which have a ‘punched out’ or ‘rat bite’ appearance and overhanging margin
- Joint space and bone density are preserved until late in the course of the disease
- Urate crystals deposited in the soft tissues form tophi and periarticular lobulated soft tissue masses
- Chondrocalcinosis may represent deposition of calcium pyrophosphate dihydrate (CPPD) crystals (pseudogout)

Gout of first MTP joint with well defined ‘punched out’ erosion with overhanging margin (arrow) and soft tissue swelling (arrowheads)
Sero-negative spondyloarthropathy
- Includes ankylosing spondylitis, psoriasis and Reiter’s syndrome; linked to HLA B27 antigen complexes
- Usually involves interphalangeal joints in an asymmetrical distribution
- Soft tissue swelling leads to dactylitis or ‘sausage digits’
- Loss of joint space and ill-defined erosions with proliferative new bone formation and periostitis
- Erosion of bone end into a sharpened pencil shape giving a ‘pencil in cup’ deformity
- Severe forms progress to ankylosis
- Fluffy new bone formation and erosions may occur at the calcaneal insertions of the Achilles and plantar fascia

Psoriatic arthropathy with new bone proliferation (arrowhead) and ‘pencil in cup’ appearance (arrow)
Synovial osteochondromatosis
- Occurs mainly in young or middle-aged adults
- Multiple metaplastic cartilaginous bodies form in the synovial membrane of a joint and become ossified
- Seen as multiple calcified intra-articular bodies, accompanied by a joint effusion
- In chronic cases, there may be pressure erosion of the periarticular bone

Synovial osteochondromatosis of the ankle joint with multiple intra-artcular ossific bodies (arrows)
Pigmented villonodular synovitis
- More recently called intra-articular tenosynovial giant cell tumour
- Most commonly seen in young adults
- Characterized by villous nodular proliferation of the synovium with haemosiderin deposition
- Dense periarticular soft tissue swelling with pressure erosion of the subarticular bone
- Joint space preserved until fairly late
- No calcification
- MRI useful to demonstrate the villous nodular synovial masses with low signal haemosiderin on all imaging sequences

PVNS with periarticular soft tissue swelling (arrowheads), bone erosion (arrow) and low signal synovial proliferation on MRI (arrows)
Septic arthritis
- Subchondral osteopenia due to hyperaemia
- Joint effusion with displacement of periarticular fat planes
- Rapid destruction of joint space
- Radiolucency and bone destruction on both sides of the joint

Septic arthritis 1st MTP joint with soft tissue swelling (arrows), loss of joint space, periarticular lucency and early osteolysis

Septic arthritis 3rd MTP joint with rapid loss of joint space and periarticular bone destruction (arrows)
ASSESSMENT OF SOFT TISSUES
Soft tissue mass
- Soft tissue mass identified on plain radiograph with distortion of soft tissue contours and increased density
- May require further evaluation with ultrasound and/or MRI

Soft tissue mass at the first MTP joint (arrowheads) corresponded to a ganglion confirmed on USS

Posterior ankle soft tissue swelling confirmed to be Achilles xanthomatosis on MRI (arrows)
Soft tissue calcification
- Vascular calcification has a linear ‘worm-like’ appearance, commonly seen in diabetics along the course of the dorsalis pedis artery between the first and second metatarsals
- Bursal calcification is most common medial to the first metatarsal head with a hallux valgus

Bursal calcification
- Post traumatic calcification within the muscles results in myositis ossificans which characteristically has dense peripheral calcification
- Neoplastic calcification may be the only indication of a soft tissue mass such as a benign haemangioma (calcified phleboliths) or malignant synovial sarcoma

Haemangioma with calcified phleboliths (arrows)
Other causes of calcification include:
- collagen vascular diseases e.g. scleroderma and dermatomyositis
- metabolic disorders e.g. hypercalcaemia and gout result in soft tissue calcification
Synovial sarcoma
- Synovial sarcoma is the most common malignant soft tissue tumour in the foot
- Up to 16% of synovial sarcomas occur in the foot
- Often presents as slow growing soft tissue mass in young adult and is often inadvertently marginally excised
- May show scattered calcification in up to 50% of cases
- No specific radiological features; it may be infiltrative with adjacent bone destruction but can also appear well defined; high index of suspicion is required
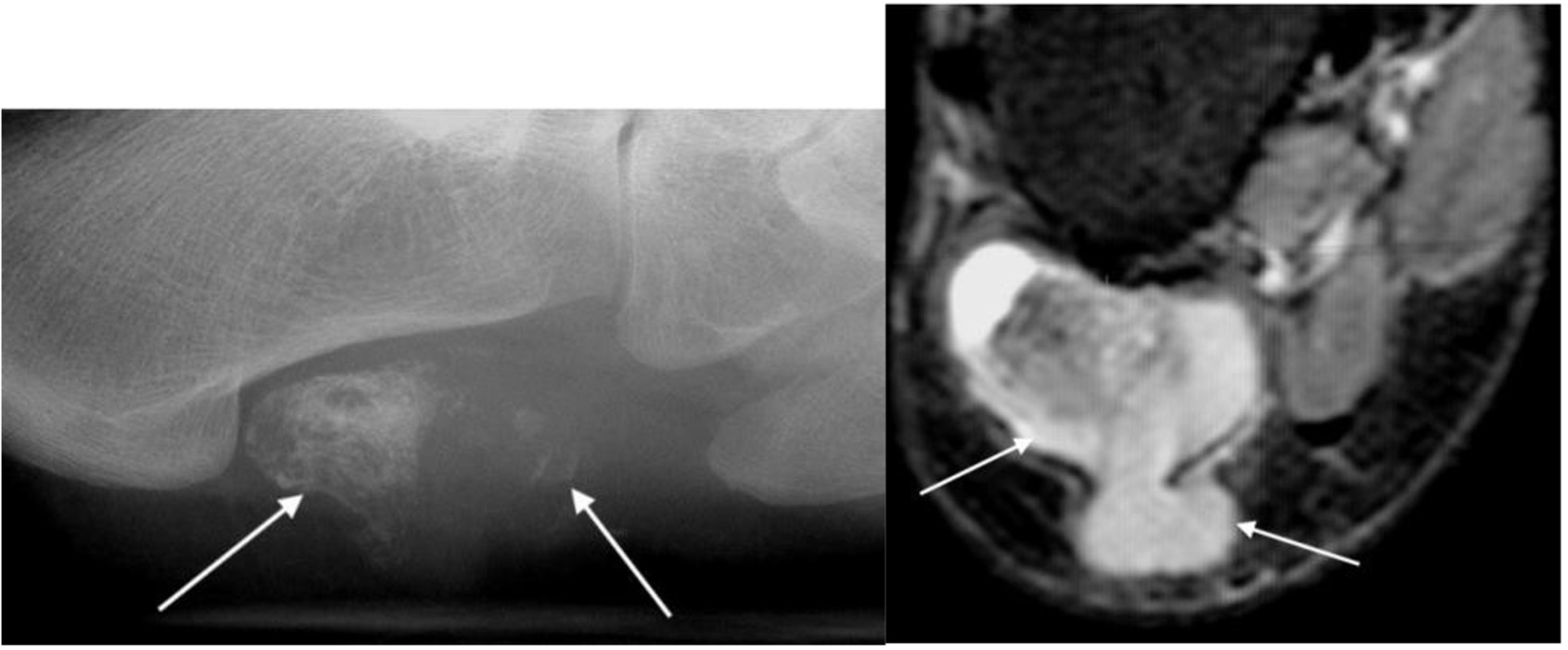
Synovial sarcoma with calcification in soft tissue mass (arrows) on plain radiograph and MRI
Foreign bodies
- Radio-opaque foreign bodies seen as areas of increased density
- More than one view is often necessary to locate the foreign body
- Glass, plastic, thorns and wood splinters are not radio-opaque and may not be seen on radiographs; ultrasound is an excellent technique for identifying these foreign bodies which are seen as linear echogenic structures

Foreign body (arrow)