Avascular Necrosis (Osteonecrosis) within the Foot and Ankle
Introduction
Avascular necrosis (AVN) within bone is a rare pathology but can affect many sites in the foot and ankle. AVN of the first metatarsal head will not be covered in this document but it is a rare, but frequently quoted, complication of correction of hallux valgus using a lateral release and a distal chevron osteotomy.
FOREFOOT
Freiberg’s Disease
Although the eponymous condition known as Freiberg’s disease has historically been viewed as a separate disease process, it shares all pathological features and some clinical and radiological features with AVN affecting other bones in the hindfoot.
- Most commonly seen in adolescence
- Preponderance in females
- 2nd metatarsal head most common; can be seen in 3rd
Blood Supply
Each metatarsal head has a dual blood supply:
- Medial deep plantar artery
- Dorsal metatarsal artery
Aetiology
Unknown but three broad theories:
- Trauma
- Impaired vascularity
- Systemic disorders
Trauma: repetitive micro-trauma, perhaps as a result of:
- anatomic anomaly e.g. relatively long 2nd MT compared to the 1st MT (Figure 1)
- deformity e.g. metatarsus primus varus
- inherent stability of 2nd MT due to the keystone articulation at its base
Impaired vascularity: approx 1/3 of the population may have an absent 2nd dorsal metatarsal artery ≈ possible poor watershed blood supply from neighbouring vessels
Systemic disorders: increased incidence in SLE, diabetes, hypercoagulable states; genetic?

Figure 1: DP radiographic view of a long 2nd metatarsal
Histopathology
Surgical appearances are classic of a punched out dorso-central lesion often with loose bodies and de-laminated cartilage (Figure 2). Histologically, most reports suggest a clear picture of AVN.

Figure 2: intra-operative findings of a central area of necrosis of the 2nd MT head
Clinical Presentation
Pain and swelling isolated to the base of the toe. Pain may be metatarsalgic in nature or nocturnal (typical of AVN). The affected toe may be elevated form the ground, swollen and, in later stages, dislocated dorsally.
Imaging
Plain standing radiographs offer a clear diagnosis in established cases (Figure 3).
CT can help define the morphology of the MT head, especially when planning osteotomies (Figure 4).
MRI can be useful in establishing a diagnosis in earlier stages of the process.

Figure 3: established changes of Freiberg’s disease within the 3rd metatarsal head
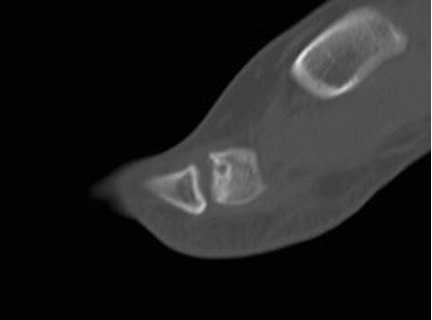
Figure 4: sagittal CT slice through the 2nd MTPJ showing the relative involvement of the dorsum of the head; this illustrates how a dorsal wedge resection osteotomy would rotate articular surface into contact with the base of the proximal phalanx
Staging
Smillie (1957) described 5 progressive stages of the disease based upon a mixture of radiographic and intra-operative findings. This staging process does not act as a tool for determining treatment.
Stage 1 - Subchondral fracture (visible only on MRI)
Stage 2 - Dorsal collapse of articular surface on plain radiographs
Stage 3 - Collapse of dorsal MT head, with plantar articular portion intact
Stage 4 - Collapse of entire MT head, joint space narrowing
Stage 5 - Severe arthritic changes and joint space obliteration
Non-operative Treatment
- Analgesia, NSAIDs
- Activity modification
- Shoe modification – stiff soles, accommodative toe box
- Orthoses – off-load the painful metatarsal head
Operative Treatment
- Core decompression – only 2 cases in the literature
- Open joint debridement
- remove loose bodies, osteophytes, and delaminated articular surface
- Metatarsal osteotomies
- dorsal closing wedge (Gauthier) – diseased area can be excised in a wedge, rotating the plantar surface into articulation with the phalanx
- shortening osteotomy (Weil type) – useful if long 2nd metatarsal
- Excision arthroplasty – risks transfer metatarsalgia and creating an unstable, short toe (Figure 5)
- Interposition arthroplasty
- rolled up EDB tendon (‘anchovy’)
- silastic replacement (Figure 6)
- more recent use of Cartiva implant with some early evidence
- Debridement, bone graft and collagen matrix
- early studies are promising

Figure 5: the sequelae of resecting the 2nd metatarsal head

Figure 6: pre and post-op silastic replacement
MIDFOOT
Avascular Necrosis of the Navicular
Blood Supply
- Dorsalis pedis and the medial plantar arteries (Figures 12 & 13)
- Indirect supply through the tibialis posterior tendon attachment onto the navicular tuberosity
- Arterial supply is radial in nature, leaving the central area of the navicular prone to avascular change – therefore centripetal intraosseous blood flow
Aetiology
Idiopathic
- Adult
- Truly idiopathic? Steroids, other risk factors (see talus section)
- Muller-Weiss disease
- Childhood
Traumatic
- Navicular is a key component of the medial column of the foot
- Apart from avulsion injuries, navicular is at risk of fracture in axial loading injuries combined with torsion or valgus / varus stresses
- Frequently high energy injuries
- Operative treatment often required to restore and balance the medial and lateral columns of the foot
- Require surgical care to prevent further injury to vascular supply:
- Consider longitudinal skin incisions and longitudinal plates (Figure 9)
- Caution with the use of circumferential anatomical plate given radial nature of blood supply (Figure 10)
- Up to 50% these fractures develop AVN to some degree
Imaging
- Plain radiographs – standing views: DP, oblique, lateral foot & AP and lat ankle
- CT – esp in trauma (Figure 7a), but also navicular stress fractures (Figure 7b)
- MRI – for foot pain of unknown origin in the presence of normal radiographs (Figure 8)
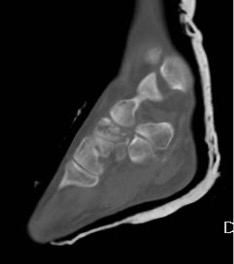
Figure 7a: CT scan demonstrates multi-fragmentary fracturing of the navicular

Figure 7b: the well-corticated appearance of a chronic stress fracture in the axial plane watershed between the medial 2/3 and lateral 1/3 of the navicular
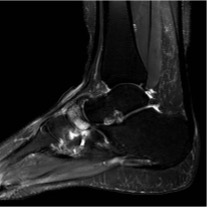
Figure 8: T2 MR image showing patchy oedema within the navicular consistent with AVN

Figure 9: Interfragmentary lag screw and bridge plating of a crushed navicular

Figure 10: Example of circumferential plating of a comminuted navicular fracture without lag screws; robust attention to preserving the medial column; late collapse of the navicular can be seen
Muller-Weiss Disease (MWD) [aka Brailsford’s Disease]
- Lateral navicular necrosis with varus alignment of the hindfoot
- Possible AVN, but not seen histologically
- Navicular is the last bone in the midfoot to ossify
- possible delay in normal ossification as aetiology
- dysplastic navicular from abnormal biomechanics in malnourished adolescents
- Late presentation of Kohler’s disease (but not persistence)
- Clinical presentation is often later due to secondary osteoarthritis
Findings
- Varus hindfoot – DP foot X-ray shows talus over calcaneus in an “apparent” flat foot
- Shortened medial column and 1st MT
- Comma (or tear) -shaped navicular (Figure 11)
- ‘Pseudo flatfoot’ – Navicular extruded medially into arch
- Knee pain (External rotated limb)

Figure 11: the classic tear-shaped navicular of MWD
Non-operative Treatment
- beneficial in high proportion
- orthosis with medial longitudinal arch support to reduce navicular sag
- shoe / orthotic lateral posting to control varus heel
- stiff rocker-soles to control arthritic midfoot joints
- steroid injection has 80% favourable response
Operative Treatment
- Decompression: not helpful
- Re-alignment: lateral displacement calcaneal osteotomy
- less common
- early stages if foot mobile
- pain not from arthritic joints
- Fusion: talo-navicular-cuneiform joints
- more common
- later stages when stiff/OA
- Correct varus by restoring column lengths with dorsal bone graft medially and/or shortening fusion of calcaneo-cuboid joint
- +/- subtalar joint fusion if too stiff to correct
Kohler’s Disease
- Typically presents between ages 2-9
- Midfoot pain
- Flattened, fragmented & sclerotic radiographic findings
- Complete resolution with cast treatment whilst symptomatic
HINDFOOT
Avascular Necrosis of the Talus
Blood Supply
In a seminal paper from 1970, Mulfinger & Trueta described the blood supply to the talus: anastomoses principally located inferiorly within the sinus tarsi/tarsal canal and from within the deltoid ligament (Figures 12&13). Sources of these anastomoses are:
- anterior tibial artery (36%)
- posterior tibial artery (47%) – main contributor to the talar body
- peroneal artery (17%)
In a second key paper, Miller et al further quantified this using MRA techniques
NB
- 60% of the talus is covered in articular cartilage
- The talus has no tendon insertions nor muscular origins
- Only ligaments insert on to the bare areas of the talus
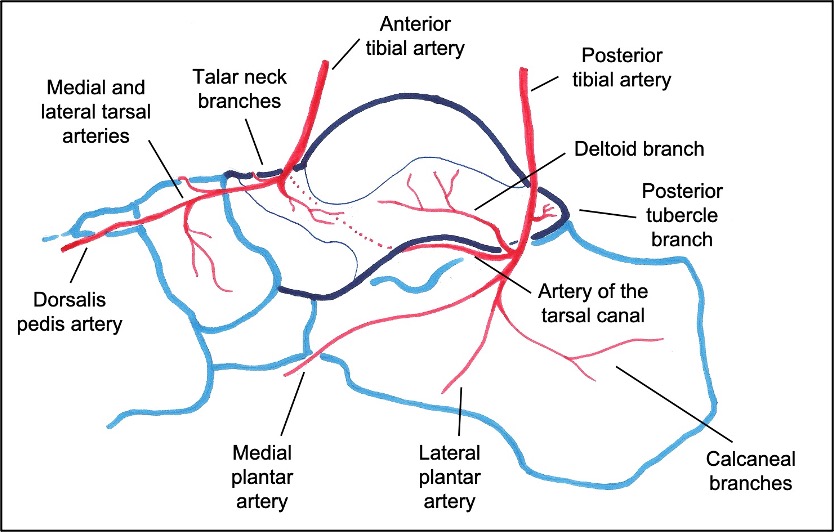
Figure 12: Blood supply to the talus, as seen from the medial side
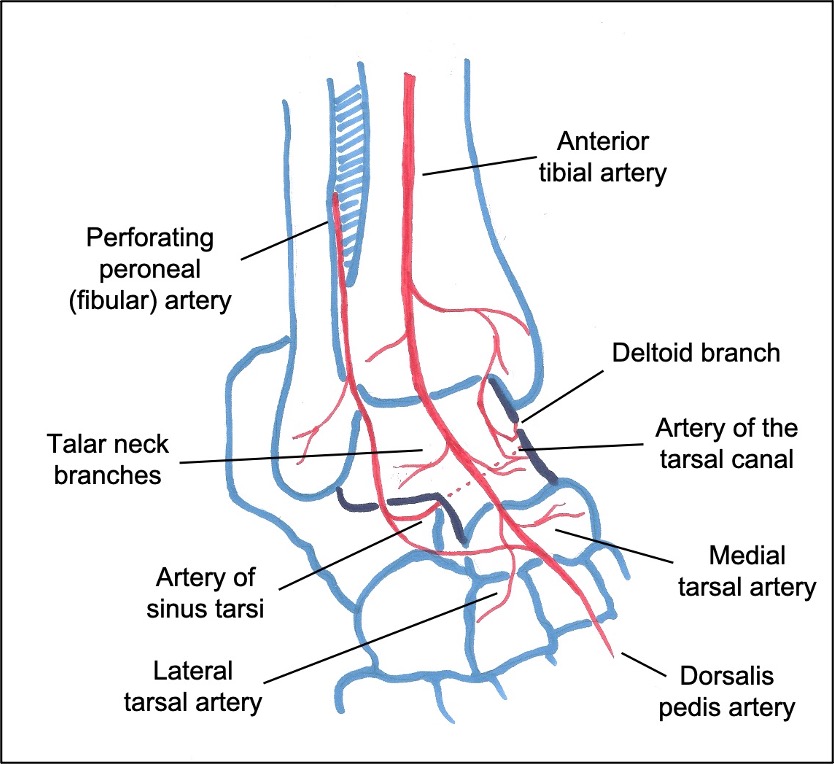
Figure 13: Blood supply to the talus, as seen from the dorsolateral aspect
Aetiology
- 75% post traumatic: fractures of the neck and/or body of talus
- 25% other aetiologies:
- steroid
- alcohol
- idiopathic
- diabetes
- SLE
- anti-retroviral therapy
- some chemotherapeutic agents
Clinical Picture
The pain from acute, evolving AVN is unremitting; rest pain is a red flag for this diagnosis. With degeneration, the pattern of pain resembles any arthrosis. Swelling is a key feature; it can resemble Charcot in the acute phase.
Deformity occurs with collapse of the talus and is thus governed by the location of the collapse. Not infrequently, the tibial plafond and calcaneus can demonstrate simultaneous areas of AVN.
Imaging
- Plain standing radiographs allow a dynamic assessment of deformity (Figure 14)
- CT to assess arthrosis & function between normal/abnormal architecture (Figure 15)
- MRI to assess disease extent, monitor progression/regression (e.g. after chemo) (Figure 16)
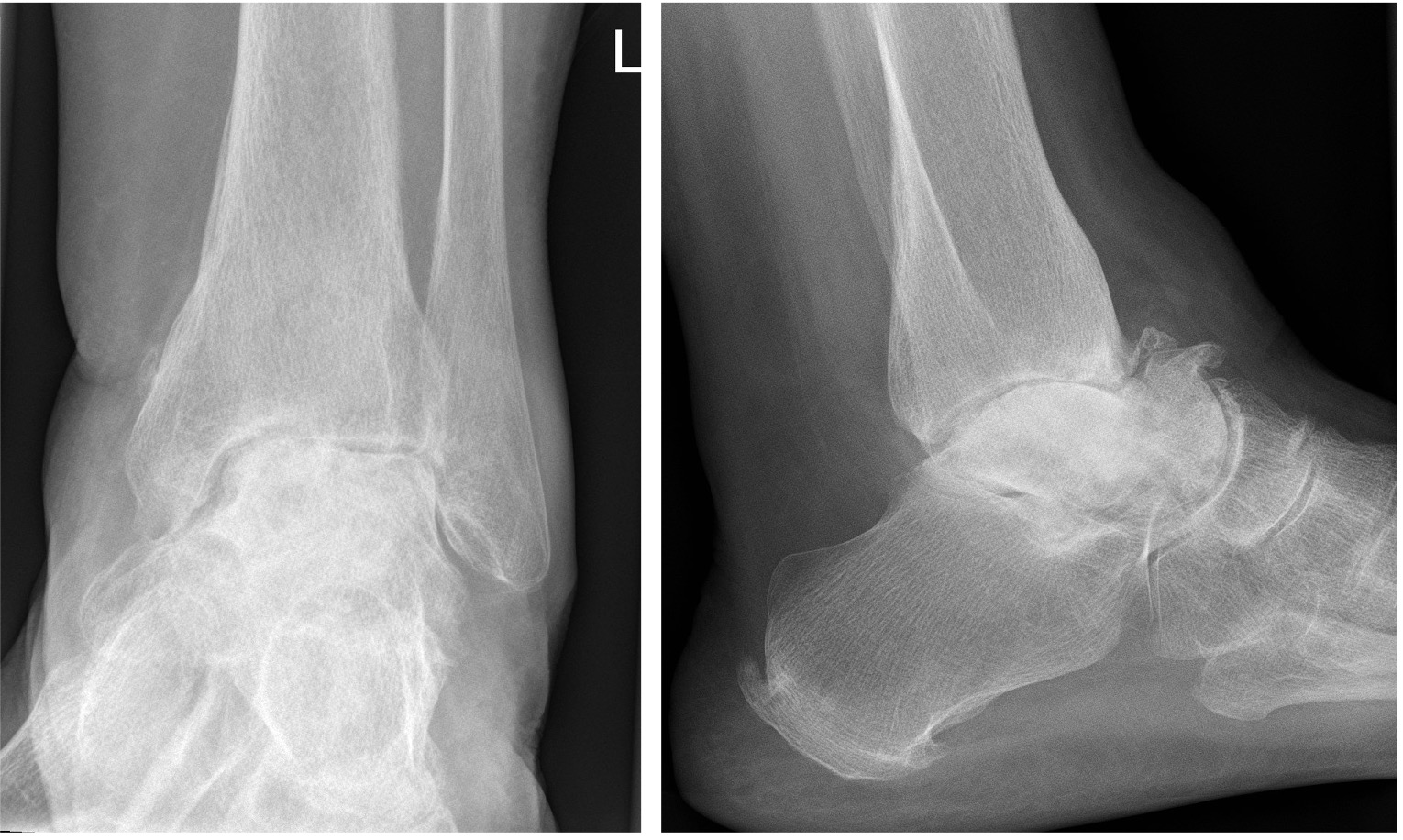
Figure 14: clear AVN of the body of the talus with arthrosis at all peri-talar joints
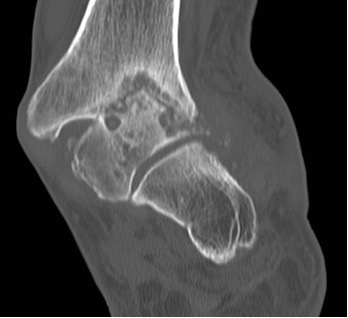
Figure 15: CT slices showing avascular necrosis of the talus and tibial plafond resulting in a severe valgus deformity
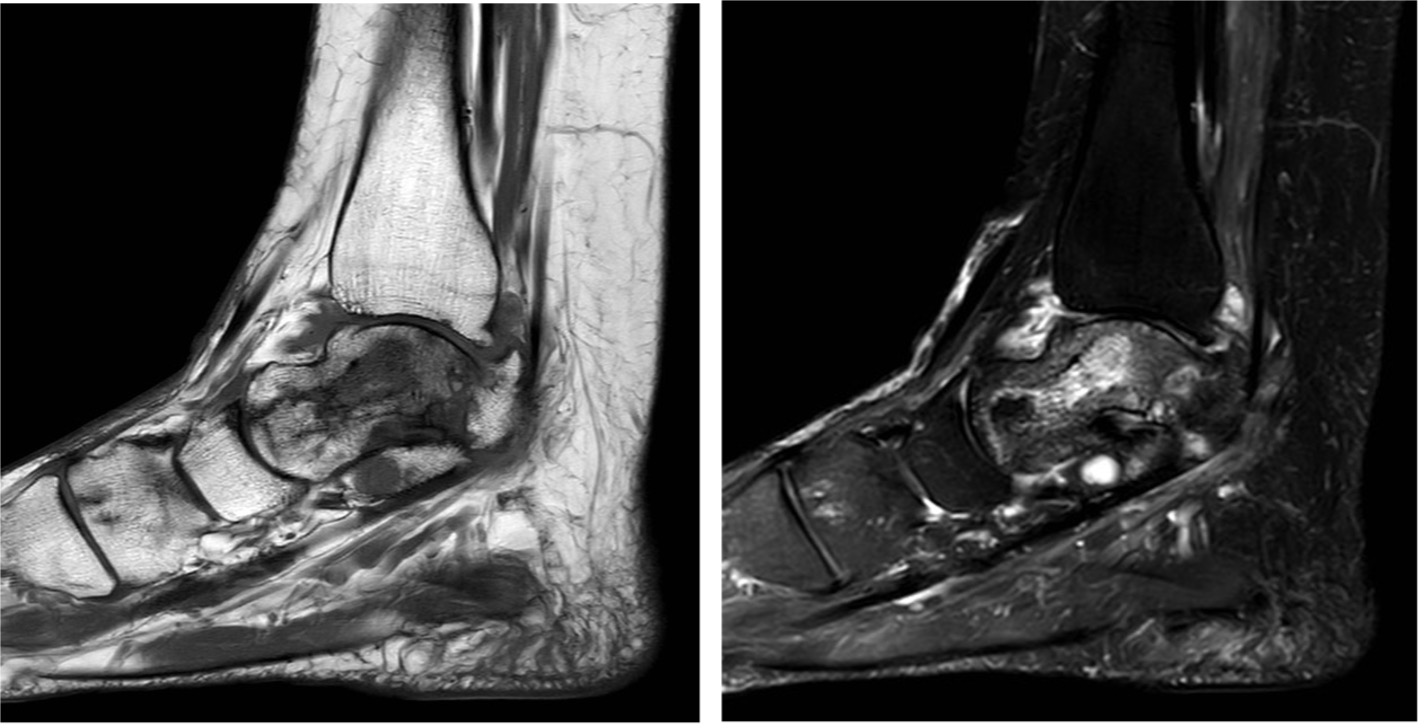
Figure 16: T1 and T2 MR images showing the serpiginous fracture lines on the T1 images and the patchy signal throughout the talus on the T2 images
Staging
Modified use of Ficat classification, stages I-IV; based upon radiographic changes
- Normal radiographs (but may have MRI changes)
- Cystic/sclerotic talus, normal bony contour, no fractures
- Subchondral collapse
- Classic features of arthrosis, collapse of the talus
Non-operative Treatment
- Analgesia, NSAIDs etc.
- Level IV evidence for the use of restricted weight bearing, use of patella tendon bearing casts and Aircast boots
- Single level I study suggests good outcome from extra-corporeal shock wave therapy in early stages
Operative Treatment
Dependent upon:
- Staging of the disease
- Plafond involvement
- Subtalar joint sparing
- TNJ sparing
- Bone loss & deformity
- Level IV evidence for use of core decompression in early stages
- Level IV evidence for vascularized/non-vascularised grafting techniques
- In cases of a spared subtalar joint and little collapse, arthroscopic ankle fusion can be offered
Tibio-talo-calcaneal fusion
- Bone loss: can use allograft (33% risk of non-union or collapse)
- other void fillers
- off-the-shelf metal spacer
- custom implants – bespoke cage to fill with bone graft
- total talar replacement
Tibio-calcaneal fusion (i.e. excision of talus)
-
- Will leave with shortened limb
- Limited anatomical options with plate/nail
- Custom-made shoe post-op (wide foot)
- Consider secondary fine wire tibial bone transport & lengthening
References
- Carmont MR, Rees RJ, Blundell CM. Current concepts review: Freiberg’s disease. Foot Ankle Int 2009: 30(2);167-176.
- Maceira E, Rochera R. Muller-Weiss disease: Clinical and biomechanical features. Foot Ankle Clin 2004:9;105-125.
- Mulfinger GE, Trueta J. The blood supply of the talus. J Bone Joint Surg 1970:52B;160-167.
- Petrie MJ, Blakey CM, Chadwick C, Davies HG, Blundell, CM, Davies MB. A new and reliable classification for fractures of the navicular and associated injuries to the midfoot. Bone Joint J 2018:100-B (2);176-182.
- Prasarn ML, Miller AN, Dyke JP et al. Arterial anatomy of the talus: A cadaver and gadolinium-enhanced MRI study. Foot Ankle Int 2010:31(11);987-993.
- Devalia K. Freiberg`s disease of lesser metatarsals treated with bone grafting and autologous matrix induced chondrogenesis (AMIC) membrane - A series of 10 cases. Foot Ankle Surg. 2023 Feb;29(2):136-142. doi: 10.1016/j.fas.2022.12.004. Epub 2022 Dec 16.