Talar Neck / Body Fracture
Introduction
Location of injury is important for management and outcome:
- Talar neck: 50%
- Talar body: 25%
- Talar process: 15%
- Talar body: <10%
The lateral talar process is generally accepted as the dividing line between the talus neck and body.
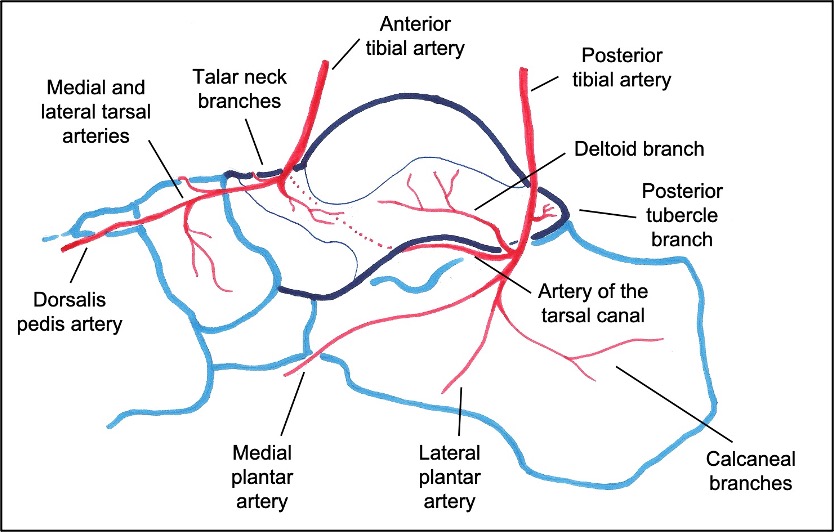
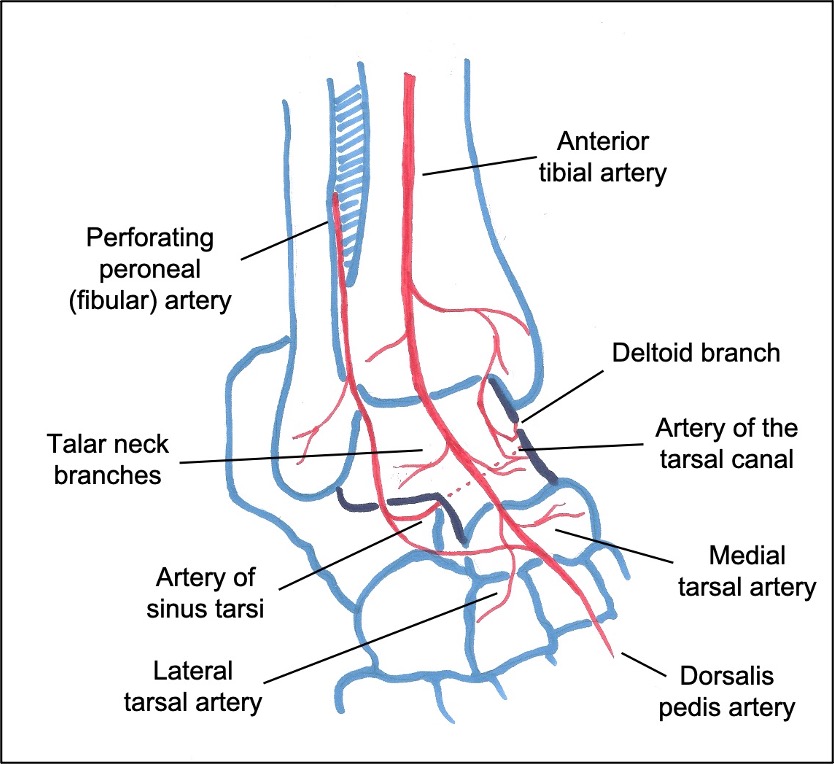
The blood supply is relatively poor because:
- 70% of the surface is covered in articular cartilage
- No muscular attachments to provide local blood supply
The anatomy of the talus blood supply:
- Deltoid branches of the posterior tibial artery supply most of the body
- Dorsalis pedis and peroneal arteries supply the lateral third and neck.
- As some vessels travel retrograde, talar neck fractures put the body at risk of AVN
Mechanism
- High-energy injuries caused by forced dorsiflexion and axial loading of the foot
- Rotational component implied by the presence of medial comminution and concurrent medial malleolar fracture (11-28%)
- Associated other fractures in ~60%
- ~ 20% are open fractures
Presentation
- Pain, deformity, bruising, swelling
- High energy mechanism – ATLS assessment and thorough 2y survey
- Neurovascular status of the foot should be assessed
- Skin tenting or skin threat
- Open fractures may involve partial or complete talus extrusion
Imaging
- Plain radiographs (AP, lateral and Canale views)
- CT scan is the gold-standard
- anatomy of the injury
- fracture extension
- comminution
- articular congruency
- occult fractures (e.g. Lisfranc, medial malleolus)
Hawkins classification
- Based on displacement and dislocation
- Further expanded by Canale and Kelly (1990), who added type IV
- The risk of AVN (%) increases with classification grade
|
Hawkins
|
I
|
Undisplaced
|
0-13%
|
|
Hawkins
|
II
|
Subtalar dislocation
|
20-50%
|
|
Hawkins
|
III
|
Subtalar & tibiotalar dislocation
|
20-100%
|
|
Hawkins
|
IV
|
Pantalar dislocation
|
70-100%
|
Management
Undisplaced fracture
- Non-weightbearing plaster cast for 6 weeks
- Weekly early radiographs to ensure no fracture displacement
- At 6 weeks, if signs of healing, convert to a walker boot with protected weight-bearing for an additional 6 weeks
Displaced fracture
Emergency Management
- High energy = ATLS principles
- In cases of skin threat or NV compromise:
- emergency reduction
- closed or open
- temporary stabilisation (cast / k-wires / ex-fix)
- If no immediate threat, recent literature suggests no difference in AVN rates with delay to reduction
- can be done the next day with appropriate surgical expertise
- when safe and with appropriate surgical expertise
- temporary stabilisation as above until soft tissues settle
- definitive fixation when safe and with appropriate expertise
- Open fractures require emergent debridement and irrigation as per BOAST guidelines
Timing of definitive surgery
- Recent literature suggests that immediate versus delayed ORIF has no significant difference in outcomes or rates of AVN
Surgical approaches
- Avoid malreduction of the talar neck in supination, pronation, or axial malalignment.
- Many authors recommend a dual anteromedial and anterolateral approach to obtain anatomical reduction
- Medial malleolar osteotomy can be added as needed and avoids jeopardising the blood supply through a posteromedial approach
- Single extended lateral approach has more recently been described
Anteromedial approach
- Incision medial to the tibialis anterior tendon
- Can extend for medial malleolus osteotomy, allowing better visualisation of body fractures and comminution
- Avoid stripping the dorsal aspect of the neck and deltoid ligament attachment to preserve the remainder of the blood supply
Anterolateral approach
- Incision lateral to the extensor digitorum longus (~1 cm above standard sinus tarsi approach)
- Adequate skin bridge if dual approach used
- Avoid injury to sinus tarsi vessels
- If used in isolation:
- extend incision up the distal fibula
- divide retinaculum and ATFL ligament (often already torn)
- allows excellent view of fracture
- allows access to – and removal of – medial comminution
- lateral fixation only
- repair ATFL (modified Brostrum)
Arthroscopic assisted reduction
- Theoretical advantages:
- reduced exposure leading to minimal soft tissue damage
- preservation of blood supply
- improved visualisation of fracture fragments
- accurate joint reduction control
- Portals:
- standard anteromedial and anterolateral ankle portals
- sinus tarsi portal in cases involving interposed subtalar fragments
- Principles:
- K-wire inserted distal to the fracture on medial aspect of the talus head to aid in reduction (joystick)
- reduction confirmed with fluoroscopy and arthroscopy
- fixation performed, usually with two cannulated screws
Fixation techniques
Screws
- Fractures can be fixed with screws used antegrade or retrograde
- Minimum of 2 screws for stability
- Biomechanical studies have suggested stronger fixation with posterior to anterior screw fixation, however accurate reduction is still imperative
Plates
- For comminuted fractures, many authors have recommended plate fixation (solid buttress or bridging strut) +/-additional screw fixation
- Can be applied to the most comminuted column: medial / lateral / both
Primary subtalar arthrodesis
- Many patients with talar neck or body fractures may require subsequent interventions, including subtalar arthrodesis
- Primary subtalar fusion may be an option in specific cases involving displaced and comminuted talar neck fractures where the progression to subtalar arthritis appears inevitable
- The primary aims would be:
- prevent progression to subtalar arthritis, pain and deformity
- avoid multiple complex procedures
- stabilise the foot by fixing the talus to an osseous strut
Postoperative management
- Most surgeons prefer immobilisation in plaster cast for first 6 weeks
- Observe for Hawkins’ sign:
- prognostic indicator of revascularisation of the talar body
- represents disuse osteopenia (can only occur if bone is vascularised)
- appears between 6 and 8 weeks
- visualised on the AP or mortise view
- absence of Hawkins’ sign does not mean AVN!
- Can progress to boot (for ankle exercises, hygiene, or night removal) but should remain non-weightbearing until there is evidence of healing, for up to 3 months
Outcomes
- Functional outcomes vary inversely with increasing Hawkins grade
- ~50% good/excellent outcomes after talar neck fracture
- ~50% poor/fair
- ~50% develop arthritis
- body > neck fractures
- subtalar > ankle OA
Complications
Avascular necrosis
- Risks:
- Greater displacement (Hawkins type)
- tobacco use
- open fractures
- ipsilateral injuries
- dual approaches
- age
- BMI
- AVN rate is 30-40% overall
- ~40% will revascularise
- ~40% will collapse
- Once AVN has been established, commence non- or partial weight-bearing to help prevent talar collapse
- Surgical management of talar AVN includes:
- drilling +/- bone grafting
- vascularised bone grafting
- adjacent joint fusion (subtalar / tibio-talo-calcaneal / pantalar) fusion
- excision of talus and tibiocalcaneal fusion with femoral head allograft (including hindfoot nail / trabecular cages)
- total talus replacement
Malunion and non-union
- ~10% malunion with talar neck fractures (usually varus)
- ~2.5% non-union
- If malunion / non-union occurs with AVN / infection:
- remove all necrotic / infected bone
- hindfoot arthrodesis with bone grafting or shortening
References
- Vallier HA, Nork SE, Barei DP, et al. Talar neck fractures: results and outcomes. J Bone Joint Surg Am 2004;86(8):1616–24.
- Srinath A et al. Talar Neck Fractures With Associated Ipsilateral Foot and Ankle Fractures Have a Higher Risk of Avascular Necrosis. J Orthop Trauma. 2024 Jun 1;38(6):220-224.
- Alley M, Vallier H, Tornetta P. Identifying Risk Factors for Osteonecrosis After Talar Fracture. J Orthop Trauma. 2024 Jan 1;38(1):25-30.
- Jordan R et al. Complications of Talar Neck Fractures by Hawkins Classification: A Systematic Review. J Foot Ankle Surg. 2017 Jul-Aug;56(4):817-821.
- Alton T, Patton D, Gee A. Classifications in Brief: The Hawkins Classification for Talus Fractures. Clin Orthop Relat Res. 2015 Sep; 473(9):3046–3049.
- Dodd A, Lefaivre K. Outcomes of Talar Neck Fractures: A Systematic Review and Meta-analysis. J Orthop Trauma. 2015 May;29(5):210-5.
- Vallier H et al. A new look at the Hawkins classification for talar neck fractures: which features of injury and treatment are predictive of osteonecrosis? J Bone Joint Surg Am. 2014 Feb 5;96(3):192-7.
- Canale ST. Fractures of the neck of the talus. Orthopedics. 1990;13:1105–1115.
- Hawkins L. Fractures of the neck of the talus. J Bone Joint Surg Am. 1970;52:991-1002.