Tendon Transfers
Introduction
What is a tendon transfer?
- Substitution of a failing muscle tendon unit (MTU) with a functional MTU
- The functioning tendon is detached from its insertion, maintaining its attachment to its parent muscle and NV pedicle, and reattached to another bone or tendon
- Aim is to correct instability, imbalance, co-ordination and improve function
Indications
Loss of function due to:
- Neurological disorder:
- Central:
- Brain (e.g. CP)
- Spinal cord injury
- CVA / stroke
- Iatrogenic (e.g. spinal surgery)
- Peripheral:
- Nerve injury (with no improvement potential)
- Charcot-Marie Tooth disease
- Trauma:
- e.g. delayed presentation of Achilles rupture
- e.g. direct injury
- Degenerative:
- e.g. tibialis posterior dysfunction →pes planus
- Rheumatoid tendon attrition
- Congenital abnormalities
General principles
- Deformity must be flexible; tendon transfer cannot overcome a fixed deformity
- Any tendon transfer loses at least one muscle grade must be good donor
- Use synergistic (in-phase) muscle where possible; helps to maintain joint balance; rehabilitate more easily
- Straight-line transfers more effective
- One function per tendon transfer
- Acceptable sacrifice of donor; must not result in loss of essential function
Other considerations
- Patient factors:
- Age (leading prognostic factor; younger patient = better outcome)
- Awareness and understanding of aims and limitations
- Motivation and compliance with post-op rehab / physio
- Time since injury
- Quality of donor (MTU)
- Quality of recipient (soft tissue bed [burns/scars] or bone quality)
- Stable underlying skeleton
- Region to be powered should be sensate
- Alternative options:
- Orthotics and bracing
- Tendon graft vs transfer for defect
- Bony correction / arthrodesis
- Amputation
Biomechanics
- Axis of tendon action
- Ankle axis = dorsi / plantar-flexion
- Subtalar axis = inversion / eversion
- Force-generating ability
- Force is proportional to cross-sectional area of muscle belly
- Amplitude is proportional to muscle length
- ‘Pennation angle’
- greater strength when muscle fibres are more parallel to the tendon
- e.g. weak interossei have high angle
- Functional phase
- swing phase (anterior compartment) vs
- stance phase (posterior and lateral compartments)
- Moment arm (see Figure 1)
- Is proportional to distance of tendon from axis of rotation
- e.g. patella increases moment arm
- Affected by tendon insertion point:
- Close to joint = small moment arm; increase motion arc but requires great strength (e.g. quads / triceps)
- Far from joint = greater moment arm; decrease motion arc but less strength required (e.g. long digit flexors / extensors)
- Excursion
- Donor MTU should have similar excursion to original
- Should be adequate to effect moment arm
- Can employ pulleys but avoid acute angles
- Can employ tenodesis effect
- e.g. toe flexors tighten as ankle dorsiflexes
- Tension
- Critical
- Fix slightly tight rather than loose
- Fixation to bone better than tendon
- Fixation at 90° into bone is preferable
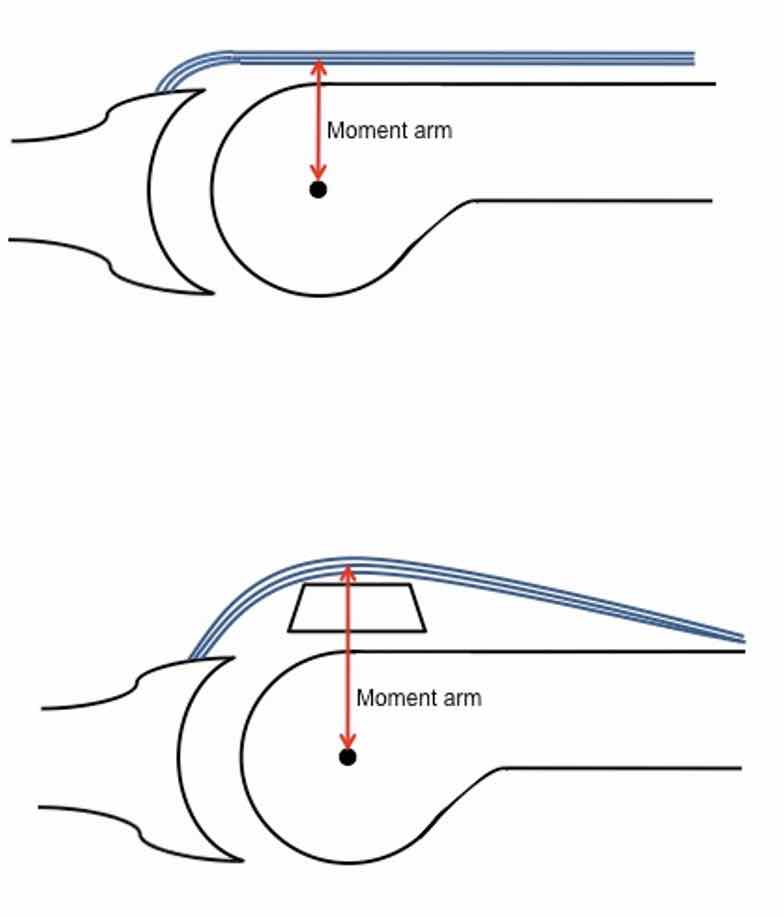
Figure 1 Demonstrates how the moment arm increases when the tendon is moved further from the axis of rotation e.g. patella (as above), sesamoid, olecranon etc. This reduces the power required to provide the same action.
Assessment
- Thorough history: injury, bracing / orthotics, progression
- Gait pattern stable or deteriorating
- Progressive or static muscle imbalance
- UMN (usually spastic) or LMN (flaccid)
- UMN harder to evaluate clinically – EMGs often useful
- Bony abnormality if deformity present from childhood
- Adult onset usually has no bony deformity
- Foot posture
- Can the foot be corrected passively to a plantigrade position?
- Are the joints fixed or flexible?
- Achilles complex tightness
- Power disparity in functioning muscles
Surgical treatment
- What are you trying to achieve?
- What function is missing?
- What is available for transfer?
Foot drop
Usually flaccid paralysis from LMN injury
- If foot does not passively dorsiflex, consider Achilles and/or posterior contracture release
- Posterior tibial tendon transfer (4 incision technique):
- Detach from navicular tuberosity
- Release c. 10cm above and posterior to medial malleolus
- Same level, just lateral to tibial crest, pass through window in interosseus membrane
- Pass subcutaneously (superficial to retinaculum) and fix into cuboid / cuneiform
- This is an out-of-phase transfer that will require physio and gait re-training (≈phase conversion)
Charcot-Marie-Tooth Disease
- Progressive, peripheral, Hereditary Motor Sensory Neuropathy (HMSN)
- Muscle imbalance:
- Tib post and peroneus longus become relatively stronger than weak Tib ant and peroneus brevis
- Result is cavovarus foot with plantar flexed first ray
- Intrinsic weakness leads to over-pull of EHL and EDL causing clawing of toes and forefoot valgus
- 'A la carte' approach: transfers would depend on which muscle groups are weak
- Surgical correction may include:
- Achilles release / lengthening
- Lateralising (+/- closing wedge) calcaneal osteotomy
- Plantar fascia release
- Peroneus longus transfer to peroneus brevis (strengthens foot eversion while reducing deforming plantar flexion of 1st ray)
- Posterior tibial tendon transfer (as above)
- EHL transfer to 1st MT head; requires simultaneous IP joint fusion (Jones procedure); converts EHL role from clawing big toe to foot dorsiflexor; corrects 1st MT flexion from big toe ‘plunger effect’ secondary to hyper-extended big toe
- Metatarsal or cuneiform osteotomies
- Lesser toe correction (see below)
Pes planus – Adult-acquired flat foot deformity (AAFD)
- Due to failure and lengthening / rupture of tibialis posterior tendon
- Surgical treatment may include:
- Medialising calcaneal osteotomy
- FDL tendon transfer:
- Detached just proximal to Knot of Henry on medial plantar side of foot
- Passed through drill hole in navicular tuberosity and sutured to self or fixed with suture anchors/interference screws or
- Sutured into tib post tendon stump (if too short for above)
- Can use FHL if FDL unavailable (Caution: consider possibility of compression of neurovascular bundle)
- Spring ligament reefing +/- artificial ligament augments e.g. Internal Brace
- Arthroereisis screw (temporary block placed in sinus tarsi to protect tendon transfer and prevent subtalar rotation); controversial
Equinovarus
- Which tendon is causing the EV deformity?
- Unopposed tibialis anterior or posterior?
- Which of these should I transfer and why?
- Use the strongest but accepting sacrifice
- Ask seated patient to push up flexed knee against your hand (‘varus confusion test’)
- Relaxes gastrocnemius complex
- Ankle dorsiflexion proves active tib ant function
- EMG studies are very useful if in doubt
- Gait analysis can also help
- In a child or younger hemiplegic patient with spastic EV deformity, tibialis posterior is the most common deforming force
- Surgery involves tibialis posterior transfer (see above) or
- Consider split tibialis posterior tendon transfer to preserve balance and prevent potential subsequent flat-foot:
- 4-incision approach:
- Medial to harvest superior half of tib post from navicular
- 5cm proximal and posterior to medial malleolus to deliver
- Corresponding incision behind lateral malleolus; pass tendon behind tibia and fibula but anterior to all tendinous and NV bundles
- Incision from base of 5th MT proximally in line with peroneus brevis
- Holding foot abducted, tenodese tib post tendon into substance of peroneus brevis
- This split transfer takes a deforming, supinating force and transforms it into a stabilising force, augmenting the peroneal pull and helping to balance the ankle
- In acquired neurological disorders, tibialis anterior is the most common deforming force due to
- Spasticity and over pull of foot invertors
- Consider a split tibialis anterior tendon transfer
- In-phase tendon transfer to provide a Y-shaped ‘yoke’ configuration to bring the lateral aspect of the foot into balance
- 3-incision technique:
- Dorso-medial over 1st MT-cuneiform joint to harvest lateral half of tibialis anterior tendon
- 8cm above ankle, lateral to tibial crest; sheath incised, tendon passer inserted proximal to distal and tendon end pulled into proximal wound; correct any equinus deformity (e.g. TA lengthening)
- Incision over cuboid; tendon passed subcutaneously (over retinaculum); inserted into cuboid – with slight over-tension – with foot held in neutral
Toe deformities
- Used for purely dynamic clawing i.e.:
- Toes look normal at rest, claw on standing
- PIPJs must be fully flexible / correctable
- Flexor Digitorum Longus tendon transfer:
- Release FDL from insertion on plantar side of distal phalanx
- Tendon split longitudinally along its natural groove
- Pass each limb up sides of proximal phalanx and suture into dorsal aspect of extensor hood with foot held in plantar flexion
- Converts flexion force of toe into extension force at PIPJ
- In-phase transfer
Achilles reconstruction
- For failed non-operative treatment of:
- Delayed presentation or ‘neglected rupture’
- Chronic Achilles tendinopathy
- Aim to restore posterior ankle stability, proprioception and heel strength
- FHL tendon transfer:
- Excise pathological Achilles tendon or fibrous scar tissue
- Short transfer: tendon harvest from postero-medial ankle at fibro-osseus tunnel, as long as possible
- Insert into calcaneus, just anterior to Achilles insertion, with tenodesis screw, foot plantigrade
- Long transfer: tendon harvest through separate medial incision at Knot of Henry
- Fix through calcaneal bone tunnel or figure-of-8 to re-connect proximal Achilles to calcaneal stump
- In-phase transfer
- MRI studies show significant compensatory FHL muscle hypertrophy post transfer
Post-operative management
- Splint / cast; elevate; DVT prophylaxis; keep joints above and below mobilised
- 2 weeks: removal of sutures
- 4 weeks: consider restricted mobilisation of single joints; protect transfer
- 6 weeks: begin gentle mobilisation of transferred tendon
- 8 weeks: commence strengthening exercises
- 12 weeks: full activity
The above is only a guide, is patient-dependant, and should ideally be managed and overseen by a dedicated physiotherapy team
Complications
- Failure / rupture / pull-out
- Tethering (particularly in poor soft tissue bed e.g. previous surgery, burns)
- Weakness
- Recurrence of deformity
- Stretching / lengthening of MTU
- Incorrect tension
- Incorrect choice of transfer
- Progressive neurological disorder
- Unstable underlying joints
Case 1


32y female. Previous attempted suicide jump resulting in left-sided pilon and calcaneal fractures. After failed non-operative treatment, underwent hindfoot (TTC) fusion with IM nailing. This failed to correct the equinovarus deformity of the midfoot (see left foot above). Then underwent successful tibialis posterior transfer from medial side to cuboid. Good clinical correction; now mobilising pain-free. Interesting example of benefit of tendon transfer after arthrodesis procedure to complete correction.
Case 2

Clinical photo taken 6 weeks following split tibialis anterior tendon transfer following iatrogenic L5 nerve root injury causing equinovarus deformity. Now balanced foot with Grade 4 power in active dorsiflexion.
MCQs
The following are typical indications for tendon transfer:
- Neurological deficit
- Fusion non-union
- Delayed presentation of Achilles rupture
- Acquired adult flat foot deformity
- Tarsal coalition
True: 1, 3, 4
The following principles are true of tendon transfers:
- Increased pennation angle correlates with increased muscle strength
- The patella reduces the moment arm of the quadriceps muscle action
- Tendons inserting closer to a joint require more muscle strength for same arc of movement
- They can be relied upon to correct skeletal instability
- They are used to restore normal power and function
True: 3
The following principles are true of tendon transfers:
- They can be combined with arthrodesis procedures to enhance stability
- They are more reliable when fixed into tendon rather than bone
- Can only be used as in-phase transfers
- Are more effective when performing multiple functions
- Assume one grade of donor muscle strength is lost following transfer
True: 1, 5