Crushed Foot
Introduction
- rare injuries but often devastating
- can be life-changing: chronic pain, deformity, stiffness, or amputation
- prognosis is often poor; early communication of this to the patient is essential
- result in both skeletal and soft tissue compromise
- leading cause of isolated foot compartment syndrome
Mechanism
- compression between two hard surfaces
- usually high-energy or polytrauma
- lower energy:
- falling heavy objects
- run over by motorised vehicles
Early Management
- The initial soft tissue insult leads to muscle ischemia followed by necrosis
- Severity and damage vary widely based on the mechanism involved
Goals of early management include:
- reducing ischemia and tissue necrosis
- preventing infection
- deciding on limb salvage versus amputation
Initial steps should follow ATLS principles. Life-threatening injuries must take precedence. Early referral to a trauma centre with orthoplastic expertise is advised (BOAST guidelines).
Management principles
- analgesia
- elevate the limb
- assess and document neurovascular status
- use Trust-approved photography to document wounds
- debride gross contamination and apply saline dressings
- initiate broad-spectrum IV antibiotics +/- tetanus
- dislocations should be urgently reduced and stabilised (splint / wires / ex-fix)
- degloving injuries can take time to declare the extent of necrosis.
- maintain high index of suspicion for compartment syndrome
Classification
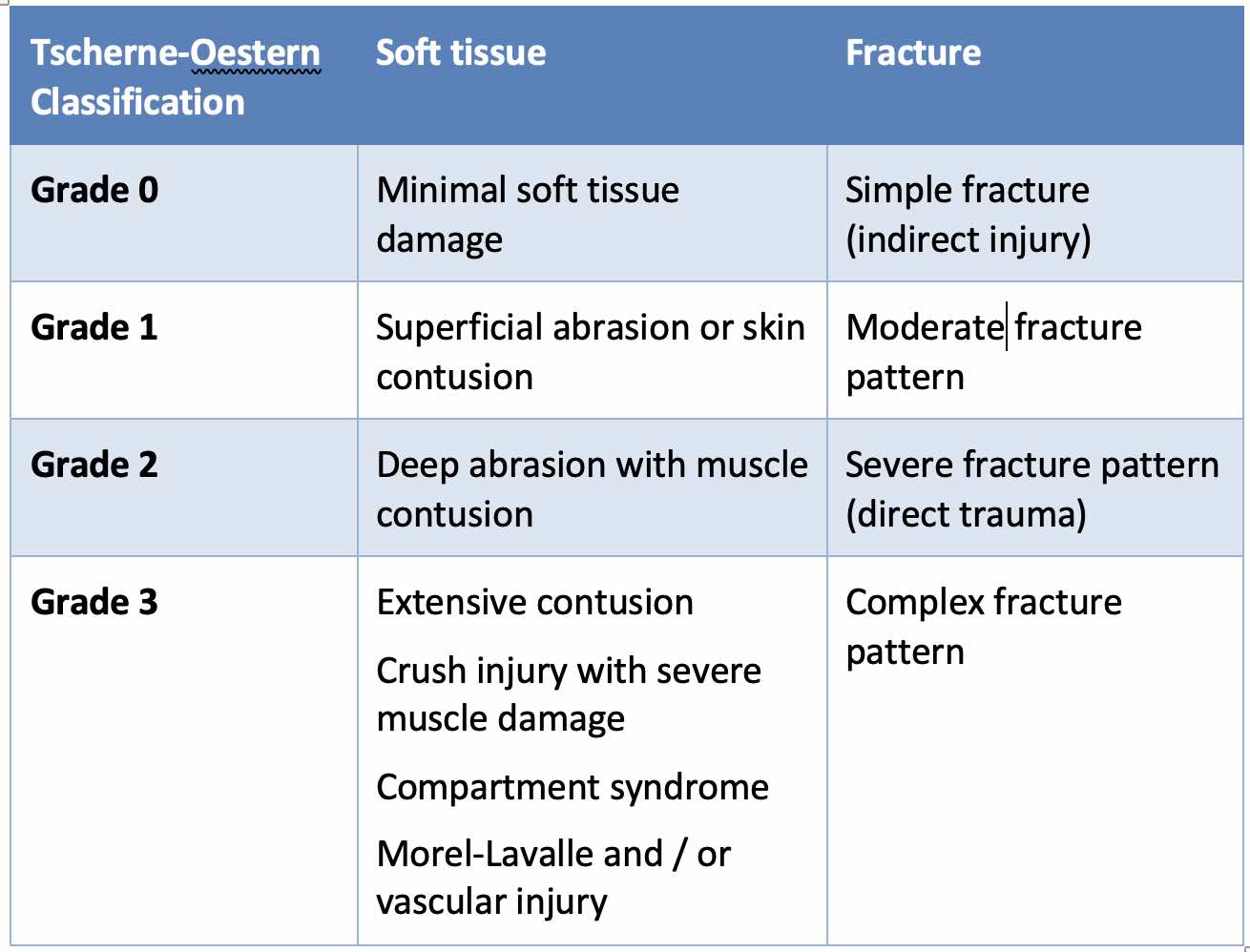
Soft tissue injuries in closed fractures can be classified by the Tscherne–Oestern system:
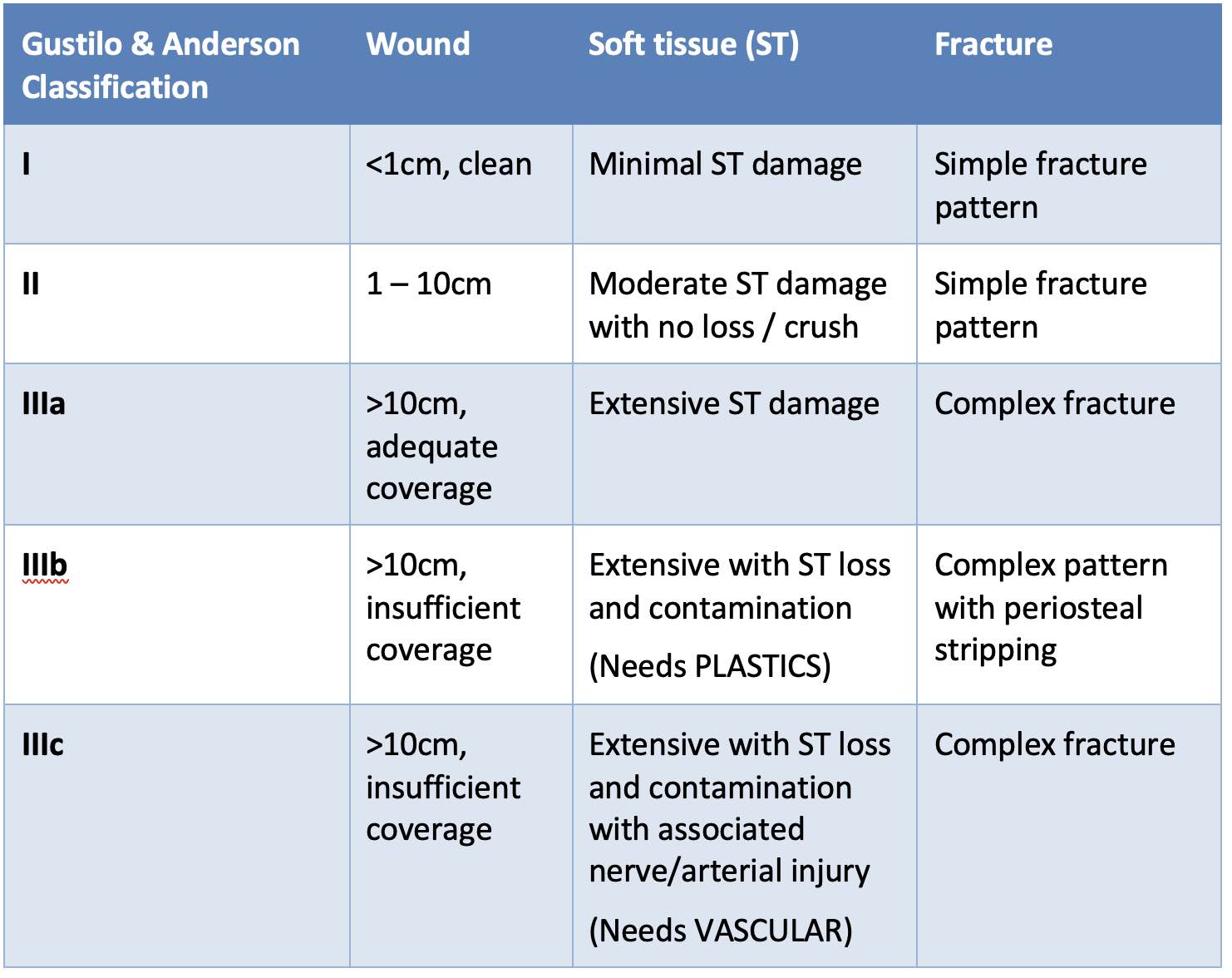
For open fractures, the Gustilo & Anderson Classification is commonly used:
In most cases of major trauma, crush injuries will be a Tscherne 3 or Gustilo Anderson III b/c.
Zwipp Score
- designed to define complex trauma of the foot and ankle
- divides the foot and ankle into five anatomical zones:
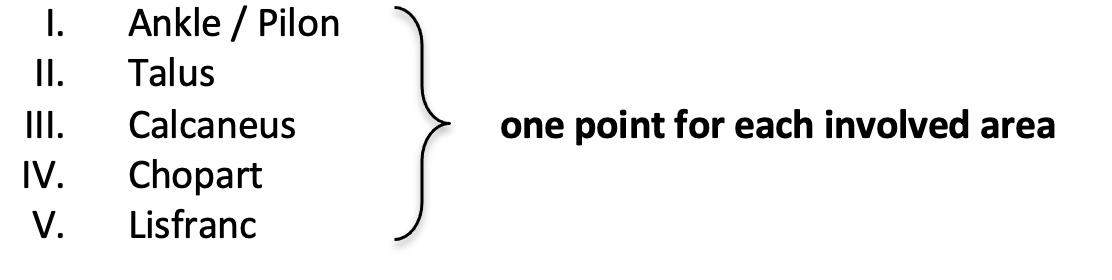
- add points based on the severity of the soft tissue injury using the Tscherne-Oestern classification (0-3)
- score ≥5 or more indicates complex trauma
- where clinicians lack expertise, even lower scores should prompt consideration for referral to a tertiary orthopedic trauma centre
Definitive Treatment
- Goal: plantigrade, pain-free foot that fits in a shoe
- MDT decision-making should include the patient and be guided by comorbidities and expectations
- Amputation rates can reach 30% in severe injuries
Reconstruction
Requires orthoplastic team collaboration. Fixation typically proceeds proximal to distal, except talus precedes ankle/pilon fixation. Restoration of length, columns, and arches is essential. Arthrodesis is recommended in complex intra-articular injuries. Nerve recovery is often poor after crush trauma.
Amputation
Indications:
- Non-salvageable limb
- Severe soft tissue and vascular damage
Goals:
- Preserve length depending on extent injury
- Restore maximal function
- Prevent pain/neuroma formation
- Allow prosthesis and early rehabilitation
For more details, see amputations page
LEAP study:
- evaluated five scoring systems in over 600 patients
- none were reliably predictive of amputation
- no functional difference was observed between amputation and salvage groups at 2 and 7 years
- both groups had poor outcomes
Others:
- more recently, the OTA-OFC score has been useful for classification of open injuries
- the Ganga Hospital Score has also been used to accurately predict lower limb amputation
Patients undergoing salvage may require multiple surgeries and face a high reoperation rate. Delayed amputation often results in worse satisfaction than primary amputation.
Conclusions
- Foot crush injuries are rare but life-changing
- Early outcome is dictated by soft tissue injury severity
- Long-term outcome is determined by bone and joint injury
- Amputation may be necessary in 30% of cases
- MDT care at trauma centres improves outcomes
References
- Schepers T, Rammelt S. Complex Foot Injury: Early and Definite Management. Foot Ankle Clin. 2017;22(1):193-213
- Godoy-Santos AL, Schepers T; Soft Tissue Foot & Ankle Group. Soft-tissue injury to the foot and ankle: literature review and staged management protocol. Acta Ortop Bras. 2019;27(4):223-229. doi:10.1590/1413-785220192704221240
- MacKenzie EJ, Bosse MJ, Kellam JF, et al. Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma [published correction appears in J Trauma 2002 Jul;53(1):48]. J Trauma. 2002;52(4):641-649. doi:10.1097/00005373-200204000-00005
- Bosse MJ, MacKenzie EJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, et al. An analysis of outcomes of reconstruction or amputation of leg-threatening injuries. N Engl J Med. 2002;347:1924–31
- Nicholls K (2021) Mechanisms and outcomes after crush injuries of the foot. Int J Foot Ankle 5:56.
- Ghoshal A, Enninghorst N, Sisak K, Balogh ZJ. An interobserver reliability comparison between the Orthopaedic Trauma Association open fracture classification and the Gustilo and Anderson classification. Bone Joint J. 2018 Feb;100-B(2):242–6. doi:10.1302/0301-620X.100B2.BJJ-2017-0367.R1.
- Rajasekaran S, Sabapathy SR, Dheenadhayalan J, Sundararajan SR, Venkatramani H, Devendra A, et al. Ganga hospital open injury score in management of open injuries. Eur J Trauma Emerg Surg. 2015 Feb;41(1):3–15. doi:10.1007/s00068-014-0465-9.