Part 1: Radiographic Views
Introduction
Plain radiographs are an important and widely available initial imaging modality of the foot and ankle and are useful for comparison with other imaging modalities.
To maximise the value of plain radiographs and to satisfy ionising radiation regulations, relevant clinical history, information sought, and differential diagnoses should be provided together with X-ray views required and whether these should be weight-bearing.
At least two views of the ankle and/or foot are required as an X-ray is a two-dimensional rendition of a three-dimensional object and pathological changes cannot be properly assessed without more than one perspective.
In general, weight-bearing views are of most use allowing biomechanical features to be deduced as well as pathological findings.
Dorsoplantar view foot (DP)

Radiographic technique
Taken either weightbearing or non-weightbearing with the X-ray beam angled 10° towards the heel (so that it is perpendicular to the metatarsals) and directed to the base of the third metatarsal.
Anatomical review areas
- General-purpose view shows the majority of the foot from the midtarsal area distally
- The neck of the talus, distal calcaneus, tarsus, metatarsals, metatarsophalangeal joints and phalanges clearly seen
- Calcaneo-cuboid and talo-navicular joints making up the midtarsal (Chopart) joint
- Tarso-metatarsal (Lisfranc) joint
- Sesamoid bones seen through the first metatarsal head
- Bodies of talus and calcaneum occluded by superimposition of the distal tibia and fibula
Dorsoplantar oblique view foot

Radiographic technique
A non-weightbearing view which may be taken in several ways. The most common method is for the patient to sit and incline the plantar surface of the foot 45° to the image receptor, with the X-ray beam directed to the base of the third metatarsal perpendicular to the dorsum of the foot.
Anatomical review areas
- Gives a distorted image of the midtarsal area but is particularly useful for the open view of the articular facets, particularly the talo-navicular, navicular-cuneiform and calcaneo-cuboid joints
- Anterior subtalar joint
- Tarso-metatarsal (Lisfranc) joints
- Difficult to see the facets of all the intercuneiform joints due to superimposition
- Good views of distal calcaneus, metatarsals, metatarsophalangeal joints and phalanges
Lateral view foot (weightbearing)

Radiographic technique
Lateral X-ray beam centred on the base of the fifth metatarsal with the side of the foot against the image receptor.
Anatomical review areas
- Trochlear surface of the talus
- Facets of the subtalar joint and calcaneum
- Calcaneo-cuboid and talo-navicular (Chopart) joints
- Sustentaculum tali and sinus tarsi are usually apparent
- Midtarsal complex is partially obscured by superimposition of the cuneiforms and metatarso-cuneiform articulations, although the first metatarso-cuneiform joint is usually seen
- The lesser metatarsals are superimposed over each other, although the first metatarsal, hallux, and first metatarso-phalangeal joint should be distinguishable
Anteroposterior view ankle (AP ankle)
Radiographic technique
Taken with the X-ray beam directed along the longitudinal axis of the foot towards the ankle, centred on a point midway between the malleoli.
Anatomical review areas
- Ankle mortise including trochlear surface of the talus, tibial plafond and malleoli
- Useful if ankle injury and avulsion fractures are suspected
- Virtually no detail of the forefoot due to superimposition
Modifications
Mortise view
- Taken with foot internally rotated 15-20°
- Projects fibula off medial tibial plafond
- Allows assessment of ankle mortise and distal tibiofibular syndesmosis
AP stress view
- Taken with foot held in inversion or eversion
- Helpful to reveal potential ligamentous and syndesmotic injuries damage
AP ankle mortice view AP ankle stress view
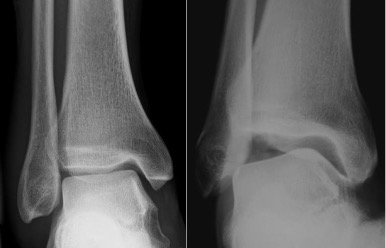
Lateral view ankle (weightbearing)
Radiographic technique
Lateral X-ray beam centred 2 cm above the inferior tip of the lateral malleolus, with the side of the foot against the image receptor.
Anatomical review areas
- Distal fibula (seen through tibia)
- Posterior lip of the tibia, also known as the posterior (or third) malleolus
- Tibiotalar and subtalar joints
- Talar dome
- Facets of the subtalar joint and calcaneum
Axial sesamoid view
Radiographic technique
Taken with X-ray beam angled towards the sesamoids with foot flexed at the metatarso- phalangeal joints. Patient may lie in a prone position with the great toe dorsiflexed and resting on the image receptor or in a supine position using a loop of bandage to retract the toes.
Anatomical review areas
- Demarcates sesamoids and their position beneath the 1st MT head on either side of the intersesamoidal ridge
- Distal lesser metatarsals also seen thus may determine whether a long metatarsal disturbs foot dynamics
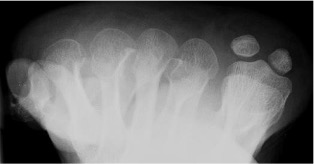
Axial sesamoid view
Calcaneal lateral view
Taken with foot in dorsiflexion and X-ray centred 2.5 cm inferior to the medial malleolus.
Calcaneal axial view
Taken with posterior ankle resting on the image receptor, foot dorsiflexed and plantar surface perpendicular to the image receptor. X-ray beam angled 40° cephalad from the long axis of the foot, centred on the base of the 3rd metatarsal.

Calcaneal lateral view Axial view