Physiology of Nerve Function Around the Foot and Ankle
- The nerves to the foot and ankle are:
- Tibial; trifurcates behind the medial malleolus into:
- medial plantar nerve: motor to small and intrinsic muscles and medial sensation
- lateral plantar nerve: motor to small and intrinsic muscles and lateral sensation
- calcaneal nerve: purely sensory to heel
- Superficial peroneal: sensory to dorsum of foot
- Deep peroneal: motor to EDB and EHB, sensory to 1st dorsal webspace
- Sural: sensory only to lateral ankle, heel and foot
- Saphenous: sensory only over medial malleolus
*awaiting image upload*
Figs 1 & 2: Sensory innervation to the foot (web images)
Nerve fibres
Nerve fibres are typically classified into A, B and C groups. Those with heavy myelination are referred to as large nerve fibres, and the thinly or un-myelinated fibres are termed small nerve fibres.

Large nerve fibres
- Fast-conducting, myelinated nerve fibres:
- central cylindrical axis surrounded by
- a myelin sheath derived from Schwann cells surrounded by
- a neurolemmal sheath
- sheaths of 2 cells meet at the node of Ranvier
- Mediate motor function (efferent tracts) and sensory symptoms (not pain and temperature)
Large fibre neuropathy:
- Symptoms: include weakness and muscle wasting
- Signs: include reduced proprioception and vibratory sense and absent deep tendon reflexes
Small nerve fibres
- Mediate thermal sensation, pain, and autonomic function
- Innervate the skin and involuntary muscles, such as cardiac and smooth muscles (autonomic)
- A delta fibres:
- thinly-myelinated
- make up ∼80% of primary sensory nerves sprouting from dorsal root ganglia
- conduct 8-20x faster then C fibres
- C fibres:
- unmyelinated and very narrow, therefore slow-conducting
- make up ∼20% of the primary afferents
Small fibre neuropathy:
- more common in the elderly; usually asymptomatic
- may cause sensory symptoms, typically:
- distal pain - burning or tingling
- itching, paraesthesia and allodynia
- symptoms usually worse at night affecting sleep
Peripheral neuropathy in the lower leg
Signs of motor involvement include foot drop, absent ankle reflexes, wasting of intrinsic foot muscles and, over time, development of pes cavus and foot deformities. Autonomic features may also be encountered e.g. lack of skin hydration.
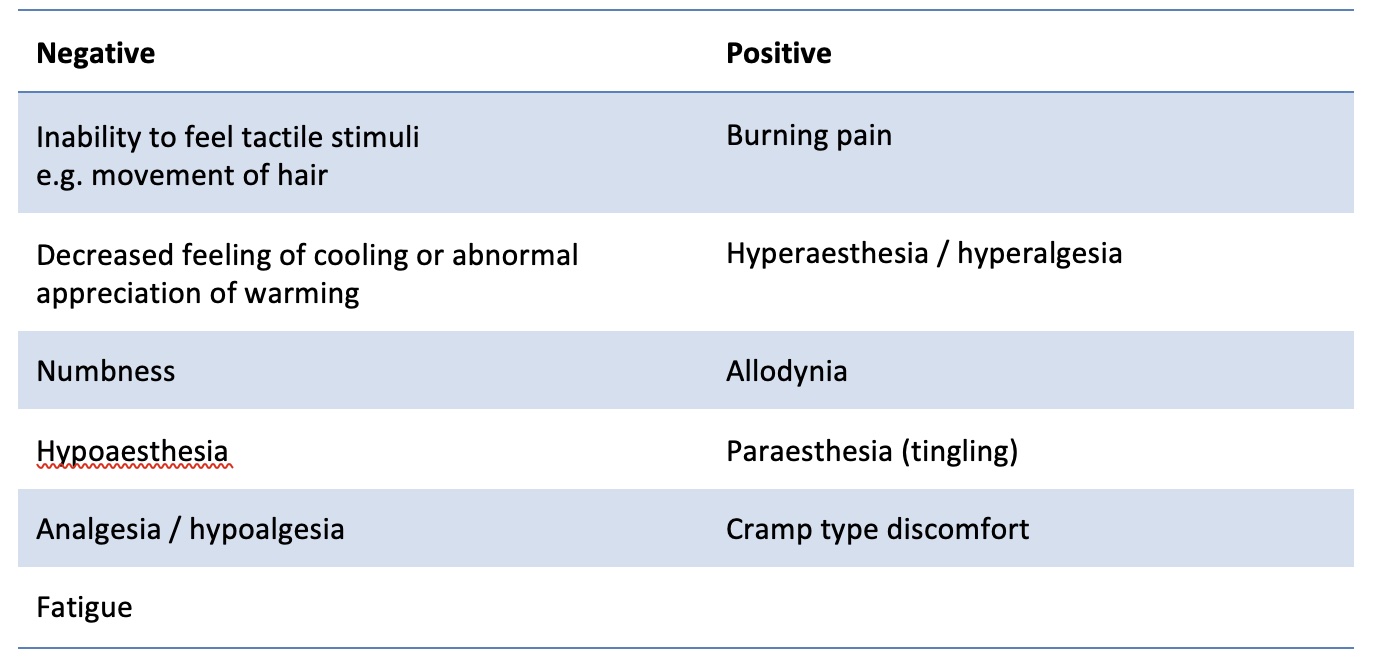
Sensory symptoms

Screening methods for peripheral neuropathy
Most recommendations for bedside neuropathy screening involve:
- light touch perception with a 10g Semmes-Weinstein monofilament
- vibration testing with a 128-Hz tuning fork
- superficial pain (pinprick) perception
- testing of deep ankle tendon reflexes
Clinical history is often sufficient, esp for conditions such as diabetes and certain rheumatological conditions. Most patients with objective evidence of diabetic peripheral neuropathy are clinically asymptomatic; they remain at risk of injury due to insensate feet.
If single-modality screening is used, monofilament light touch or vibration testing appears to be more sensitive and specific than superficial pain (pinprick) or ankle reflex testing. Light touch with a cotton swab is often substituted for monofilament testing in busy clinical practice but its sensitivity and specificity in isolation is unknown.
Confirmatory diagnosis
Electromyography (EMG) and nerve conduction studies (NCS) are useful to:
- confirm the suspected diagnosis
- exclude mimickers (e.g. S1 radiculopathy, carpal tunnel syndrome)
- localise the process (length dependent, length independent, multifocal)
- confirm the modalities affected (sensory, motor)
- define whether the neuropathy is secondary to axonal loss, demyelination, or both
- define the severity of the neuropathy
NCS can usually only assess large fibres.
Assessment of small fibre neuropathy (SFN) often requires referral to a tertiary service:
- skin biopsy measurement of intraepidermal nerve fibre density is the current gold standard
- non-invasive methods such as corneal confocal microscopy, quantitative sensory tests and laser-doppler imaging, amongst other techniques, are available
Importance of patient age when interpreting results
There is an age-related decline in neuronal function, with some modalities greater affected.
For example, with vibration sensation, almost a quarter of those aged > 65 years and one-third of those > 75 years have reduced vibration sensation on clinical examination.
Likewise, although a vibration perception of 25 volts has been considered as the threshold for ‘insensate feet’ in many diabetic foot ulcer studies, a threshold lower than 25 volts in a younger individual should also be viewed with suspicion for peripheral neuropathy.
When would a neurology consult be useful?
- In patients with rapidly progressive neuropathy with significant functional deficit
- In patients with multifocal or asymmetrical involvement
Patients with diabetic neuropathy are best cared for within the diabetic foot multidisciplinary setting; access to such units is widely and easily available.
Differential diagnosis
- Alcohol abuse or nutritional deficiency (e.g. post bariatric surgery)
- Diabetes of any duration (most common cause in UK), impaired glucose tolerance
- Drug-induced, esp after chemotherapy
- Chronic kidney disease
- Vitamin B12 / folate deficiency
- Hereditary neuropathies (e.g. Charcot-Marie-Tooth)
- Inflammatory (e.g. CIDP – chronic inflammatory demyelinating polyradiculoneuropathy)
- Paraneoplastic (malignancy or monoclonal gammopathy)
- Thyroid disease
- Spinal canal stenosis
- Autoimmune (e.g. vasculitis, Sjögren’s, sarcoid)
- Infection (HIV, Hep B/C, syphilis, Lyme’s, Guillain-Barré, Covid)
Entrapment neuropathies
Posterior tarsal tunnel syndrome:
- compression of the posterior tibial nerve
- fibro-osseus tunnel behind the medial malleolus
- causes neuropathic symptoms to the heel and under the foot into the toes
Anterior tarsal tunnel syndrome:
- entrapment of the deep peroneal nerve
- beneath the thin inferior extensor retinaculum at the ankle
- or more distally at the lateral and medial terminal branches over the TNJ and CCJ
- pain radiating to the first dorsal web space
Distal tarsal tunnel syndrome:
- entrapment of the first branch of the lateral plantar (Baxter’s) nerve
- often misdiagnosed initially as plantar fasciitis
Medial plantar nerve compression:
- seen most often in running athletes (Jogger’s foot)
- compression at Knot of Henry (where FHL and FDL cross)
- pain radiating to the medial arch
Sural nerve:
- most vulnerable 15mm distal to tip of fibula when foot rests in equinus
Morton’s neuroma:
- enlargement at point of digital nerve bifurcation
- compression between adjacent metatarsal heads
References
Watson JC, Dyck PJ. Peripheral Neuropathy: A Practical Approach to Diagnosis and Symptom Management. Mayo Clin Proc. 2015 Jul;90(7):940-51. doi: 10.1016/j.mayocp.2015.05.004.
Vas PR, Sharma S, Rayman G. Distal Sensorimotor Neuropathy: Improvements in Diagnosis. Rev Diabet Stud. 2015 Spring-Summer;12(1-2):29-47. doi: 10.1900/RDS.2015.12.29.
Ferkel E, Davis WH, Ellington JK. Entrapment Neuropathies of the Foot and Ankle. Clin Sports Med. 2015 Oct;34(4):791-801. doi: 10.1016/j.csm.2015.06.002.