Ankle Fractures in Diabetic Patients
Introduction
Ankle fractures in diabetic patients require special consideration in their assessment, treatment and management.
Diabetic patients account for ~12% of all ankle fracture patients.
Increased risk of complications due to:
- reduced bone mineral density (in T1 diabetes)
- reduced bone quality due to accumulation of advanced glycosylation end products (T1 and T2)
- increased falls risk due to neuropathy and eye disease
Complications include infection, Charcot, mal-union, non-union, amputation and death; patients must be counselled appropriately.
Risk stratification
The risk of complications increases with severity of disease.
Compared to non-diabetic patients:
- NIDDMs have a modest increase in infection risk after ankle fracture surgery:
- 1.14 relative risk of deep infection
- 1.72 relative risk of osteomyelitis
- IDMMS have a greater increase in complications:
- 2x risk of post-op infection
- 10x risk of osteomyelitis
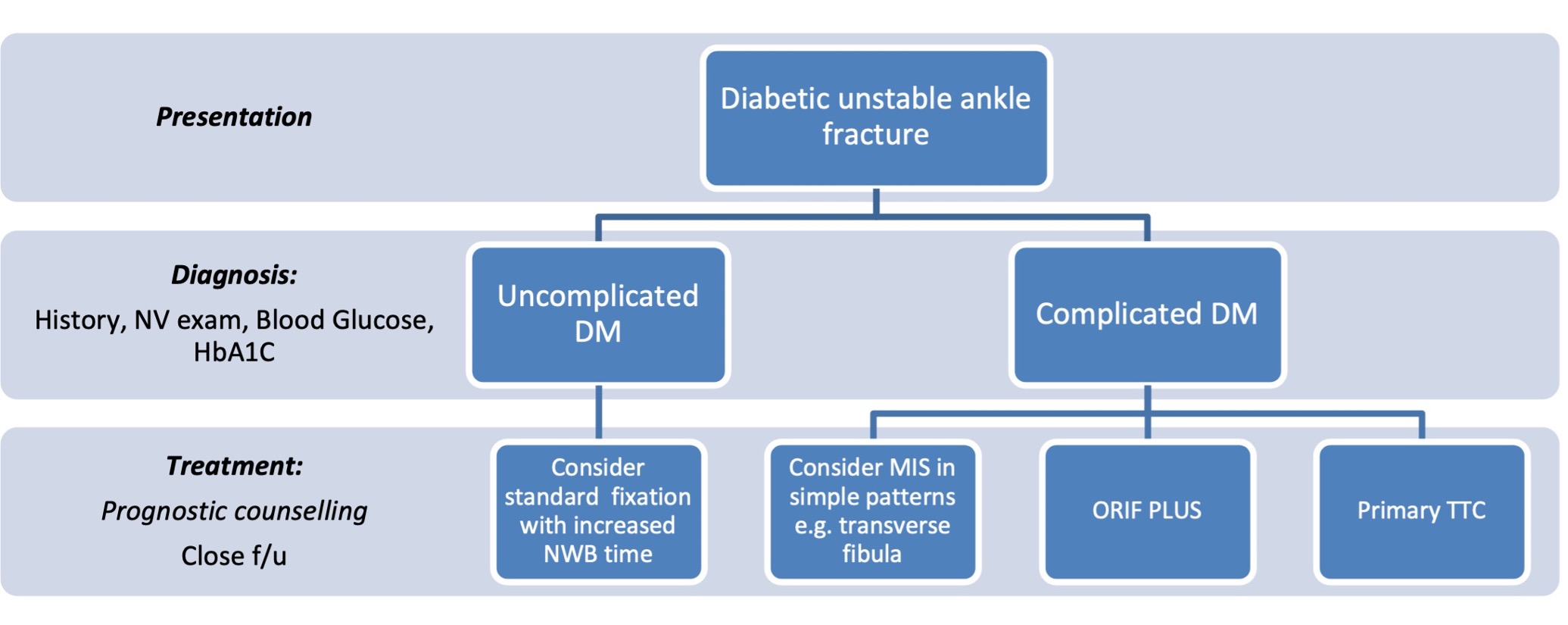
Complicated diabetes can be defined as the presence of:
- peripheral neuropathy
- peripheral arterial disease
- and/or advanced diabetic nephropathy
The highest rates of complications are in this cohort; they must be identified at initial assessment.
Assessment
History must include evaluation of features associated with complicated diabetes; if the patient has been able to bear weight on an unstable ankle fracture prior to presentation, this should alert to possible peripheral neuropathy.
A thorough neurovascular assessment should be performed as peripheral arterial disease and neuropathy are associated with the highest risk of complications including amputation;
- pulses are often difficult to palpate with an acute fracture due to swelling
- bedside Dopplers or vascular assessment may be helpful prior to surgery
- ABPI may be falsely elevated in the diabetic patient due to arterial calcification
Hyperglycaemia impairs bone healing. Furthermore, ankle fracture surgery in diabetics can itself lead to rises in blood glucose which are sustained for many months. Blood glucose and serum HbA1C should be obtained in these patients with early liaison with anaesthetists and the diabetic team to ensure optimisation of control, both perioperatively and in the longer term.
Treatment
Non-operative treatment by casting in unstable ankle fractures in diabetic patients is not recommended:
- associated with up to 21-fold increased risk of complications compared to operative treatment:
- loss of reduction
- development of Charcot
- progression of deformity
- ulceration and deep infection
- high rates of secondary surgery
Augmented fixation or ‘ORIF plus’ is the mainstay of treatment for unstable diabetic ankle fractures.
Principles include:
- use of multiple tetracortical syndesmotic screws
- longer segment fixation
- use of locking plates
- consideration of transarticular pins to improve stability

Example of "Fibula pro-tibia" technique. Medial side left alone due to severe soft tissue compromise.
Minimally invasive techniques – including fibular nailing or cannulated screws – may be considered in appropriate fracture patterns where there is concern about surrounding soft tissues.
Primary arthrodesis with tibio-talo-calcaneal nailing may be considered in complex patients; high rates of limb salvage have been demonstrated with this technique.
Wound closure may be augmented with vacuum-assisted dressings in high-risk patients.
Post-operative
Given the impairment of bone healing in diabetics, a doubling of NWB period has traditionally been recommended to allow for slower union. However, recent small studies have demonstrated an acceptable complication profile with early protected weight-bearing after wound healing.
Close follow-up is required with increased frequency of outpatient visits and serial x-rays to monitor for development of Charcot, loss of reduction, wound complications and infection.
Summary flowchart
References
Liu JW, Ahn J, Nakonezny PA, Lalli T, VanPelt MD, Raspovic KM, Wukich DK, Liu GT. Insulin Dependence Increases the Risk of 30-Day Postoperative Complications Following Ankle Fracture Surgery in Patients With Diabetes Mellitus. J Foot Ankle Surg 2021. 20:S1067-2516(21)00091-0
Lovy AJ, Dowdell J, Keswani A, Koehler S, Kim J, Weinfeld S, Joseph D. Nonoperative Versus Operative Treatment of Displaced Ankle Fractures in Diabetics. Foot Ankle Int 2017. 38(3):255-260
Nash WJ, Hester T, Ha J. Current concepts and challenges in managing ankle fractures in the presence of diabetes: A systematic review of the literature. J Clin Orthop Trauma 2021. 3;17:44-53
Wukich DK, Joseph A, Ryan M, Ramirez C, Irrgang JJ. Outcomes of ankle fractures in patients with uncomplicated versus complicated diabetes. Foot Ankle Int 2011. 32(2):120-30.