Part 6: Bone Tumours
BENIGN BONE TUMOURS
- Well defined, often sclerotic, margin
- Expansile lesion may result in cortical thinning but no cortical destruction
- A periosteal reaction may be present which appears uniform and solid
Enchondroma
- Benign cartilaginous tumour
- Typically found in the diaphyses of the metatarsals and phalanges
- Well defined, radiolucent and mildly expansile with cortical thinning
- May have internal calcification
- Multiple enchondromas (as seen in Ollier’s disease) may have malignant potential

Multiple enchondromas (arrows) in Ollier’s disease
Osteochondroma
- Cartilage-capped exostosis seen as a bony outgrowth
- Cartilaginous component invisible on plain radiographs unless calcified
- Rarely, the cartilage cap may undergo transformation to malignant chondrosarcoma; cartilage cap thickness > 2cm is suspicious and usually assessed on MRI
- Pedunculated, subungual exostoses on the distal phalanx of the hallux are common and usually have a cartilaginous cap, classifying them as osteochondromata

Osteochondroma of first proximal phalanx (arrow)
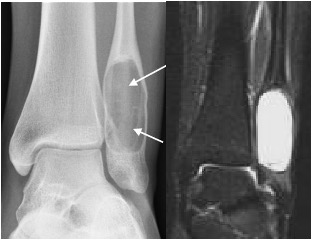
Intraosseous lipoma
- Typically occurs in the calcaneum
- Well-defined lucent lesion; may contain central calcification
- MRI diagnostic to confirm fatty matrix, seen as high T1 and T2 signal which supresses with fat saturation

Intraosseous lipoma calcaneum
Fibrous cortical defect
- Common, up to 20 % of immature skeletons
- Caused by fibrous tissue from the periosteum invading the underlying cortex; may be related to a subclinical injury
- Usually an incidental finding
- Seen as a cortically-based, radiolucent lesion with well-defined sclerotic border in the tibial metaphyses
- Larger lesions (>2cm) that expand into the medullary cavity are referred to as non-ossifying fibromas

Fibrous cortical defect with well-defined sclerotic margin
Solitary (simple) bone cyst
- Cyst of unknown origin containing clear or serosanguinous fluid
- Occurs in the immature skeleton
- May occur in distal tibia / fibula, calcaneum and long bones of the foot
- Seen as a well-demarcated, radiolucent intramedullary lesion with cortical thinning
- May present with a pathological fracture
Simple bone cyst distal fibula seen as well-defined, slightly expansile lucent lesion
Aneurysmal bone cyst
- Usually in patients <30 years
- Sponge-like cyst with blood-filled spaces and fibrous septae; may arise as the result of a vascular anomaly
- Seen as radiolucent, often rapidly expansile lesion with a thin cortical shell
- Matrix fluid-fluid levels on MRI are typical
Aneurysmal bone cyst with fluid-fluid levels on MRI
Osteoid osteoma
- Typically in young patients who complain of severe rest and night pain
- Dramatic relief with aspirin
- Seen as ovoid radiolucent nidus up to 1cm in diameter surrounded by sclerosis and periosteal thickening
- Sclerosis may mask the radiolucent nidus on plain radiographs; best seen on thin CT sections

Osteoid osteoma with radiolucent nidus (arrows) and surrounding sclerosis best seen on CT
Giant cell tumour of bone
- Occur primarily in the mature skeleton
- Typical eccentric epiphyseal location, extending to subarticular surface
- Seen as radiolucent lesion with well-defined, but non-sclerotic, margin
- May be expansile with cortical thinning
- Approximately 15% of giant cell tumours are malignant

Giant cell tumour of distal tibia seen as eccentric expansile epiphyseal lucent lesion (arrows)
MALIGNANT BONE TUMOURS
- Ill-defined margin
- Permeative, ‘moth-eaten’ appearance
- Cortical destruction
- Periosteal reaction has lamellated (‘onion-skinned’) or spiculated (‘hair on end’ or ‘sunray’) appearance
- Soft tissue mass: distortion of adjacent soft tissue contour with increased density; may have calcification
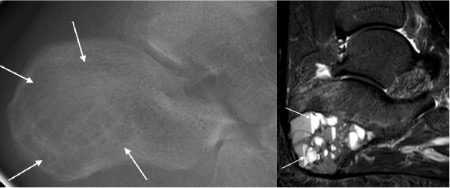
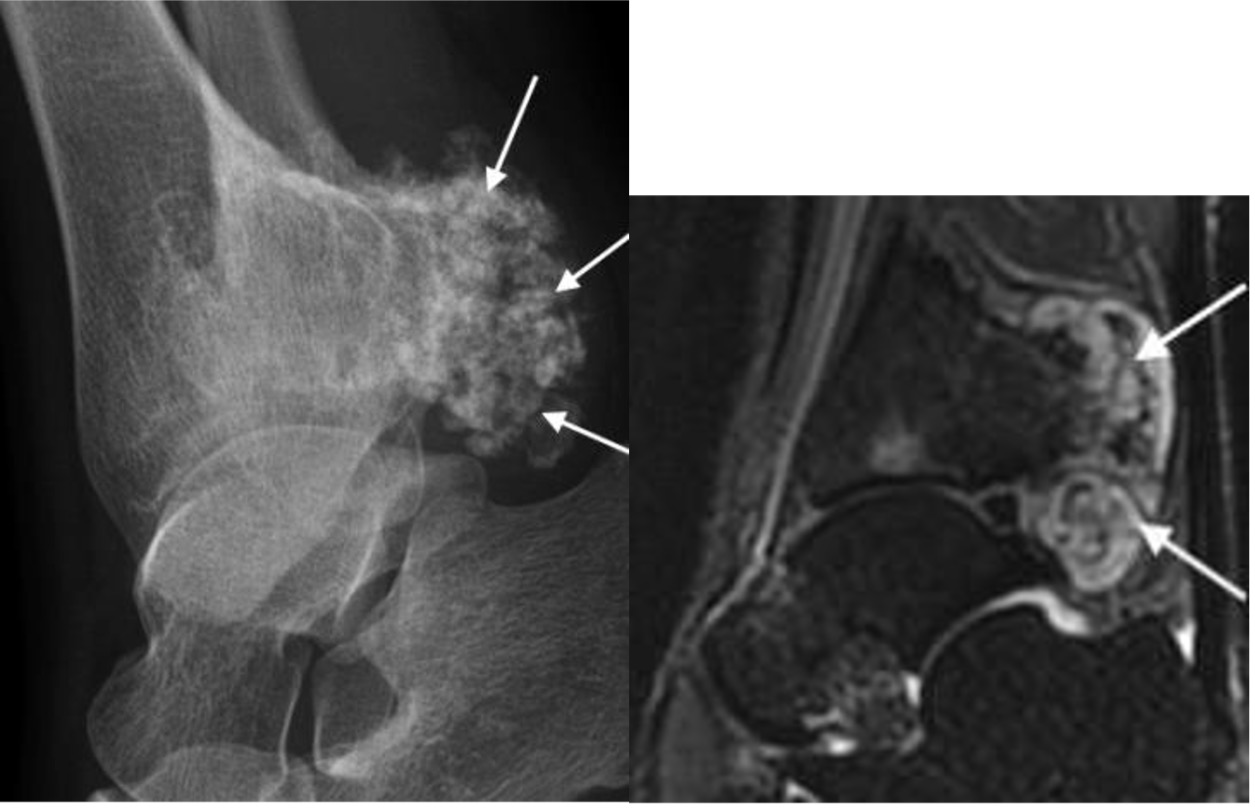
Osteosarcoma
- Uncommon in the foot
- Typically occurs in immature skeleton; may occur in older age group usually secondary to Paget’s
- Seen as ill-defined, often mixed lytic and sclerotic lesion
- As tumour osteoid becomes mineralized, there is increasing sclerosis and new bone formation with a ‘cloud-like’ density
- Aggressive periosteal reaction with wedge of ossified tissue under the periosteum called a Codman’s triangle
Osteosarcoma calcaneus with sclerosis on xray (left) and low signal on MRI (right) due to osteoid formation
Ewing’s sarcoma
- Occur in immature skeleton
- Seen as an ill-defined, permeative lesion in diaphysis of a long bone or within a flat bone
- Often has cortical destruction and spiculated periosteal reaction
- Osteomyelitis has a similar radiographic appearance
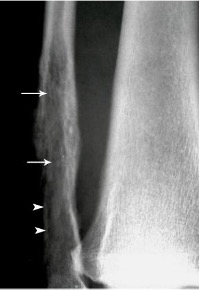
Ewing’s sarcoma with ill-defined, permeative infiltration of fibula (arrows) and cortical destruction (arrowheads)
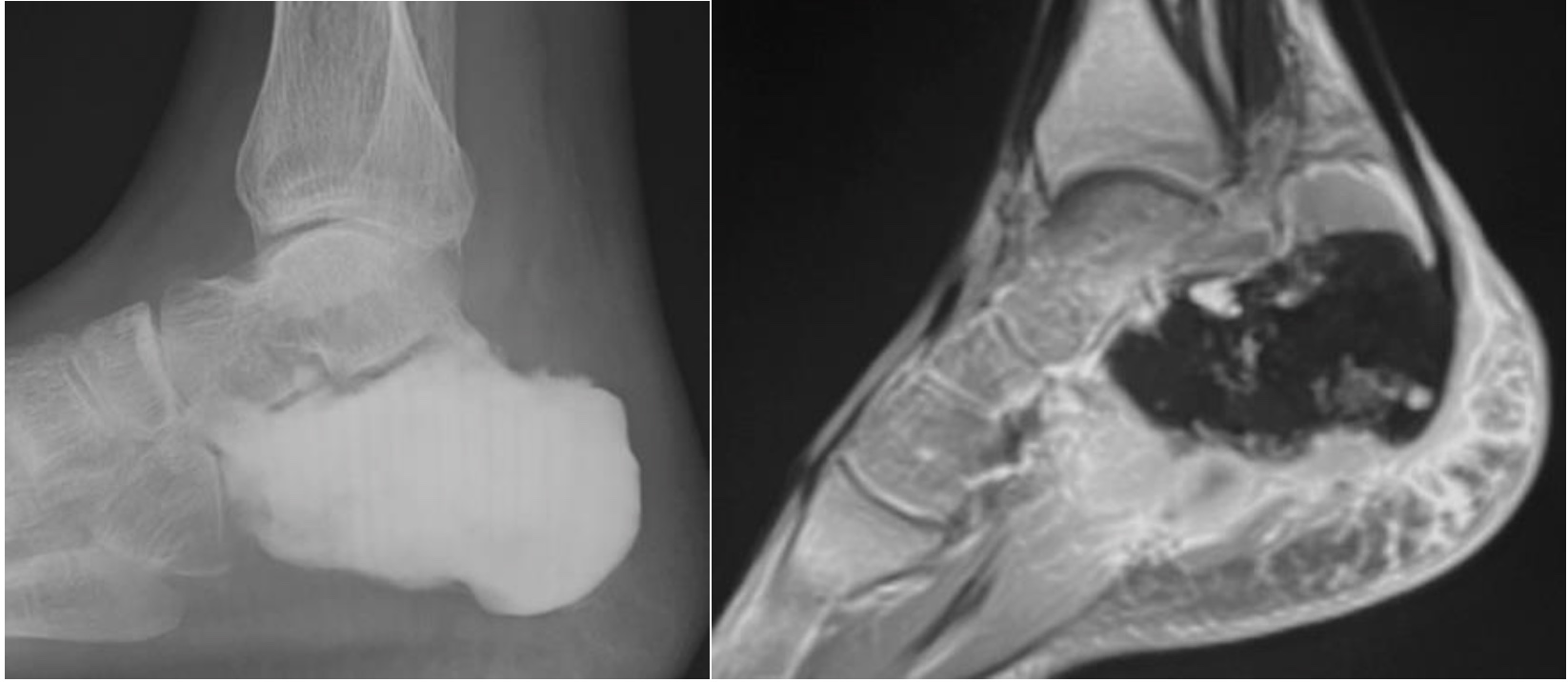
Chondrosarcoma
- Cartilaginous tumours are rare in the foot but have been noted in the calcaneum
- Occur in the mature skeleton ~50-70y
- Usually contain calcification which has a ‘popcorn’ or ‘snowflake’ appearance indicative of their cartilaginous origin
Chondrosarcoma posterior distal tibia with ‘popcorn-like’ chondroid calcification (arrows)
Metastases
- Needs to be considered in the differential diagnosis of any lytic lesion in a patient >40 years
- Metastases to the foot are most commonly from primary lung carcinoma
- Usually lytic, destructive lesions
- Sclerotic lesions most commonly prostate and breast metastases
- Thyroid and renal metastases produce expansile lesions
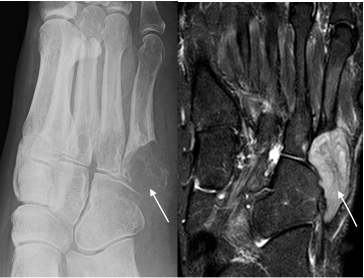
Metastasis base 5th metatarsal seen as lytic destructive lesion (arrow) in patient with known lung carcinoma