The Role of Osteotomies in the Management of Ankle OA
Introduction
- Ankle osteoarthritis (OA) represents ~1% of all OA globally
- 80% are post-traumatic: lower leg fractures and/or repeated ankle sprains
- The ankle joint is highly congruent and carries around 4x body weight in the stance phase
- The cartilage of the ankle joint is thinner than that of the hip and knee, but can withstand greater shear and tensile forces, enabling lower contact pressure; this helps to explain why symptomatic ankle OA is 9x less common than knee OA
- Perfect alignment in ankle OA is rare; patients with end-stage ankle OA often present with a concomitant deformity:
- supramalleolar (varus 28%, valgus 8%)
- intra-articular
- inframalleolar (varus 22%, valgus 19%)

Figure 1. Supramalleolar valgus deformity

Figure 2. Intra-articular varus deformity
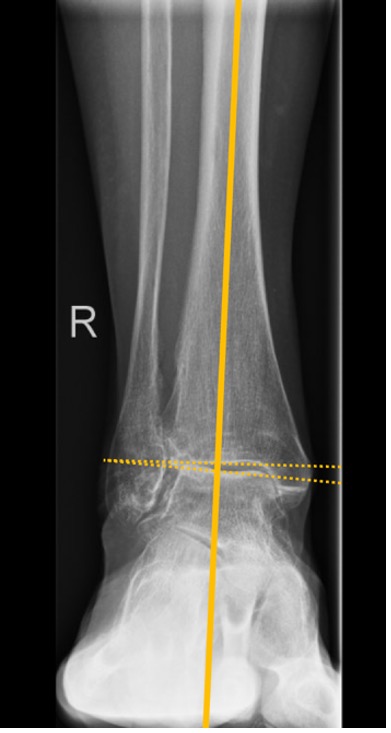
Figure 3. Intra-articular valgus deformity
Supramalleolar osteotomy (SMO)
Aims
- restoration of the lower-leg axis
- improve intra-articular load distribution
- slow down (or stop) degeneration of the tibiotalar joint
Indications
- incongruent ankle OA (varus or valgus) with intact medial or lateral tibiotalar joint cartilage
- alignment correction of severely deformed, end-stage ankle OA before (or at the same time as) total ankle arthroplasty
For which grades of arthritis can SMO be used?
- increasing levels of arthritis (Takakura grade) lead to higher 5y failure rate (defined as conversion to ankle arthrodesis or replacement)
- significantly higher failure rate from grade 3a to 3b
- 3a where obliteration of the joint space is limited to the gutter
- 3b where obliteration of the joint space extends to the roof of the talar dome
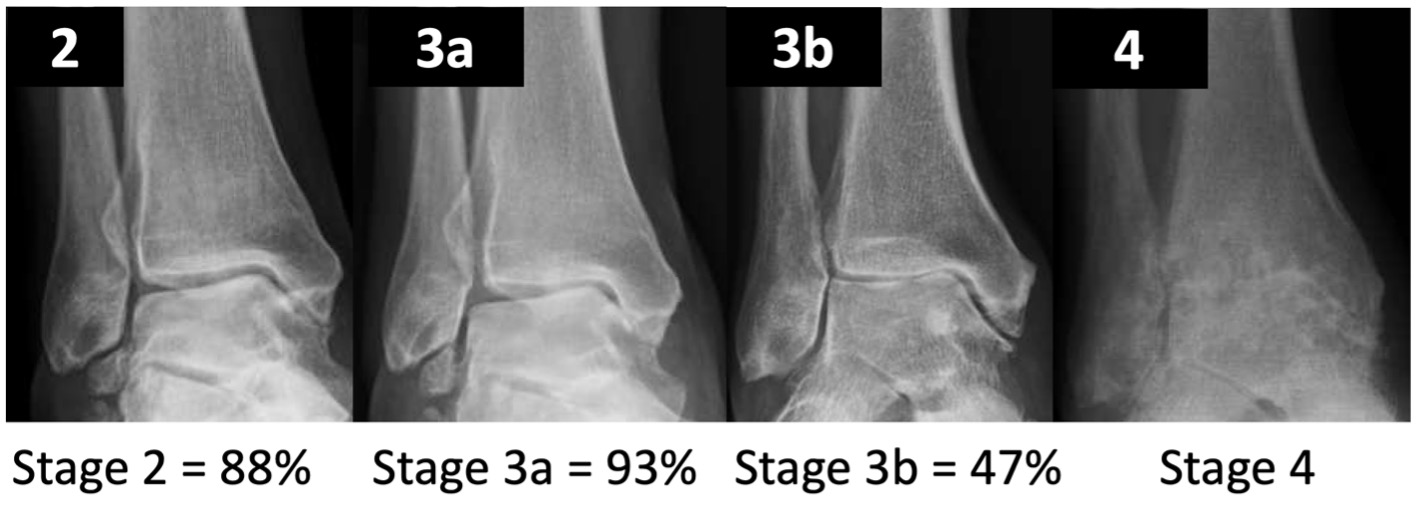
Figure 4. 5-year failure rate of SMO (conversion to TAR or AA)
Absolute contraindications
- hindfoot instability that cannot be managed with ligament reconstruction
- severe vascular or neurological insufficiency
- neuroarthropathy
- acute or chronic infection of the ankle
- non-compliance
Relative contraindications include
- elderly patients with impaired bone quality or frailty
- advanced tibiotalar OA
- tobacco smoking
- long-term steroid medication
- severe osteoporosis
- rheumatoid or inflammatory disease
- uncontrolled diabetes
Types of osteotomies for ankle arthritis include:
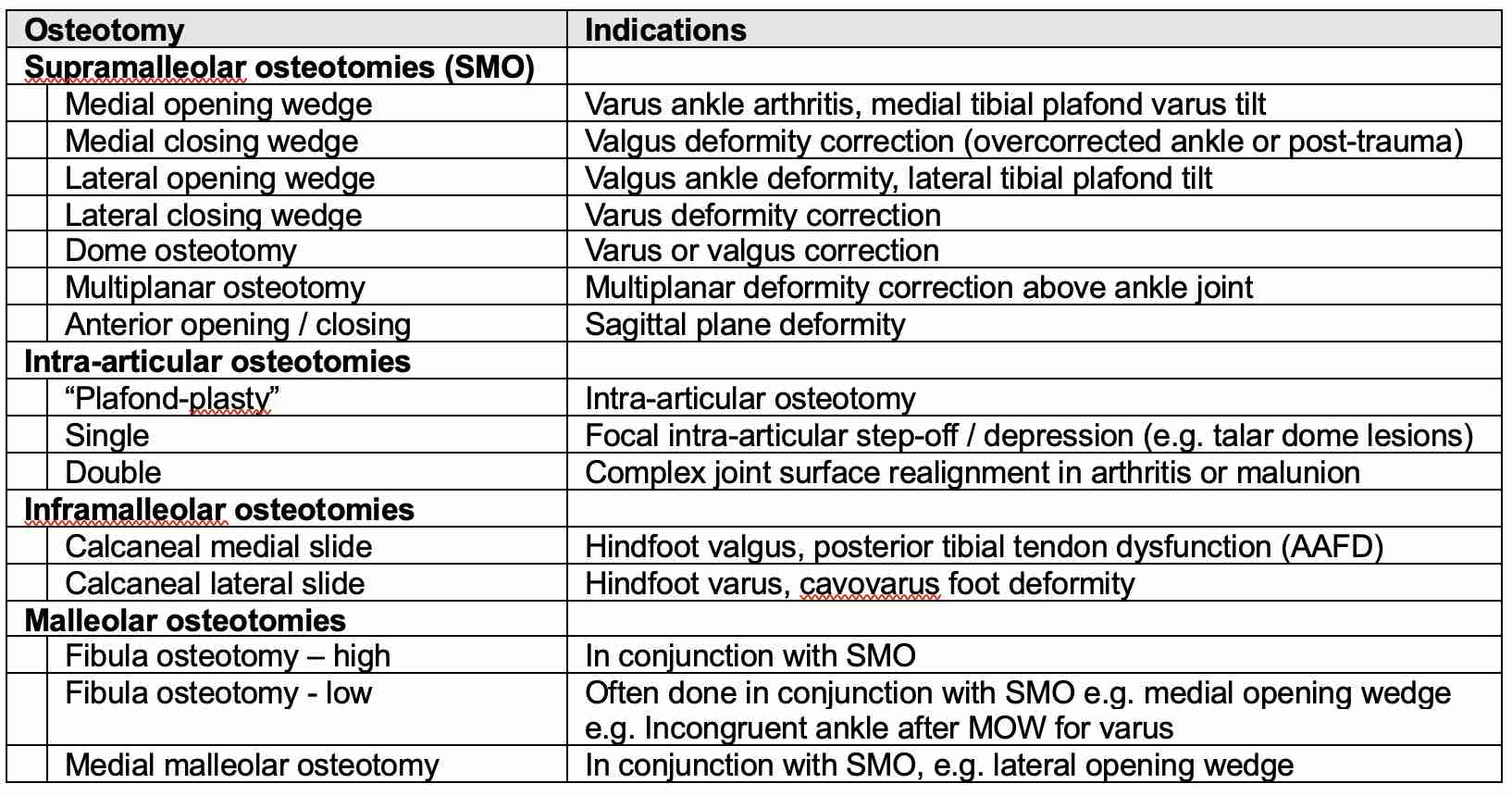
- Supramalleolar osteotomies are most commonly used
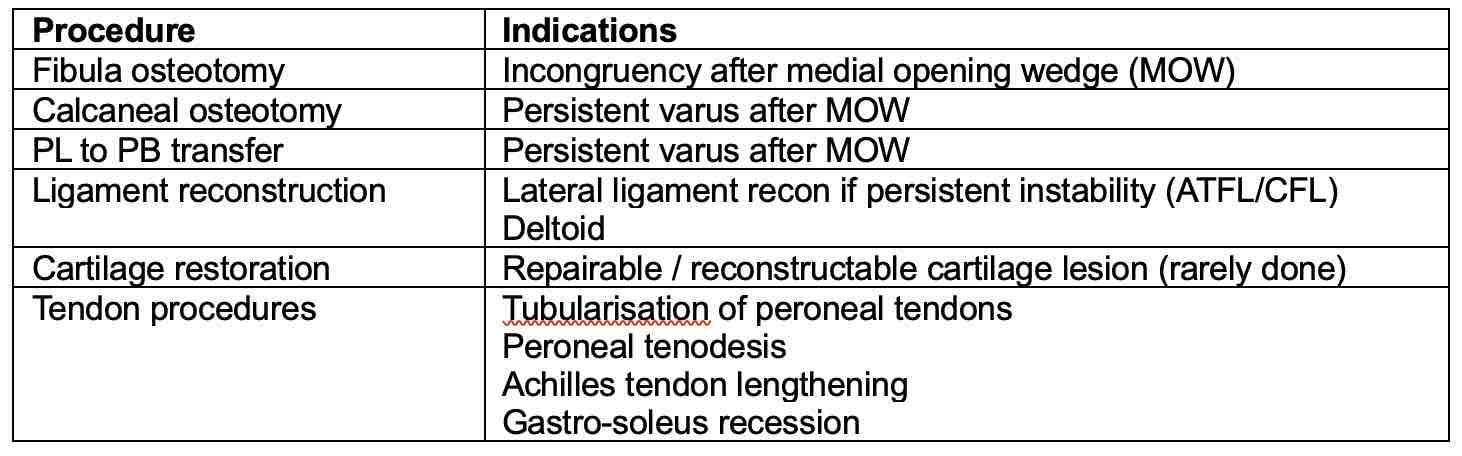
- Osteotomy combinations or adjuvant procedures may also be done to correct deformity and stabilise the ankle
- These include:
Imaging
- Weight-bearing radiographs:
- ankle AP, lateral and mortise views
- whole leg alignment views (to assess proximal deformities and to guide surgical planning)
- hindfoot alignment views can also be beneficial
- CT (weight-bearing if poss):
- assessment of degenerative changes in the tibiotalar and adjacent joints
- MRI or SPECT CT may also be useful to assess adjacent joints
Preoperative Planning
- angles are measured using a weight-bearing mortise view
- coronal plane parameters:
- medial distal tibial angle (MDTA), also called the tibial articular surface angle (TAS)
- tibio-talar surface angle (TTS)
- tibio-talar angle (TTA)
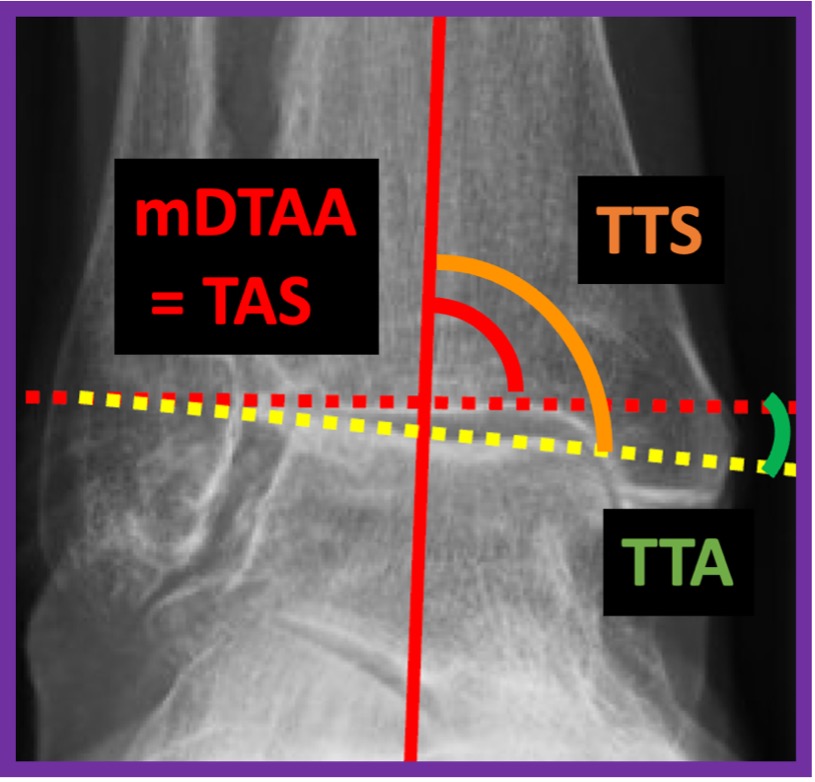
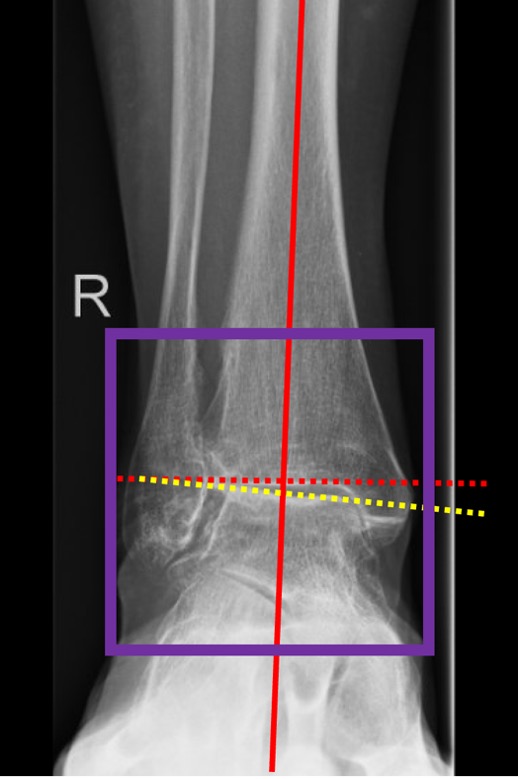
Figure 5. Measuring the deformity
- MDTA (TAS) is crucial for quantifying the supramalleolar deformity (Fig. 3)
- TTA normally defines the centre of rotation of angulation (CORA)
- Talar tilt should be used for quantitative assessment of an intra-articular deformity in the coronal plane. It is defined as the difference between the MDTA and the TTA
Talus tilt (TTA) = TTS – mDTAA
- Values of >4° are considered to be pathological
- The hindfoot alignment view should be used for quantitative assessment of an inframalleolar deformity in the coronal plane
- For calculating the degree of operative correction, the following formula is used to determine the required amount of opening or closing of the osteotomy:
H = tan α₁ x W
-
- H is the height of the wedge
- α₁ is the amount of deformity, incl approx 2°-4° of desired overcorrection
- W is the width of the distal tibia
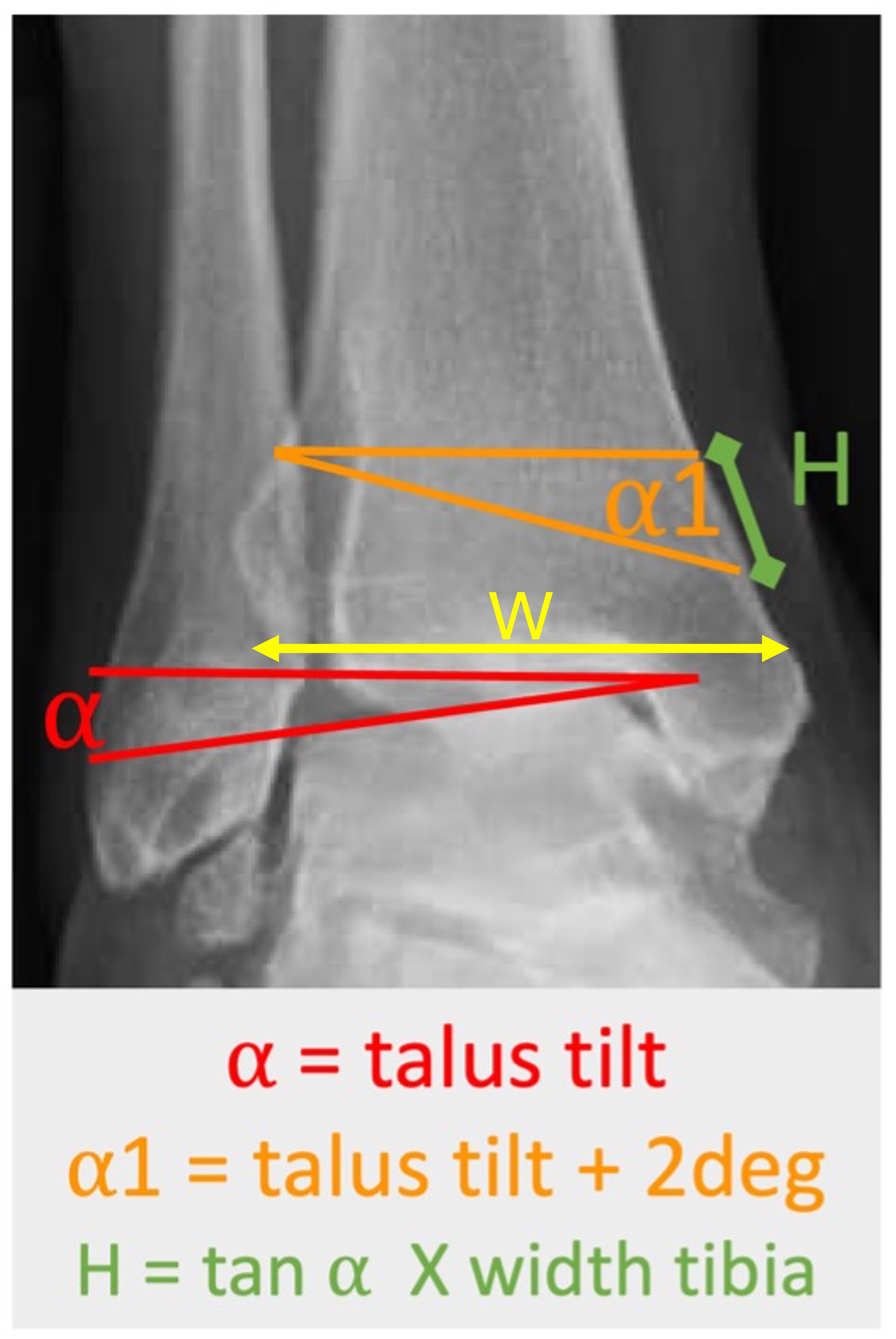
Figure 6. Calculation of the opening or closing wedge dimensions
Surgical technique
- General and/or regional anaesthesia can be used
- Supine with the ipsilateral pelvis lifted to correct for external rotation of the foot
- Limb exsanguination and a thigh tourniquet can be applied unless contraindicated
- Anterior ankle arthroscopy can be performed to assess / treat OCDs
- 3 main options to correct varus / valgus deformity of the ankle:
- opening wedge osteotomy
- closing wedge osteotomy
- focal dome osteotomy
Lateral osteotomies are technically more difficult due to the proximity of the fibula. However, if >10° of correction is needed, a lateral wedge osteotomy is often preferred.
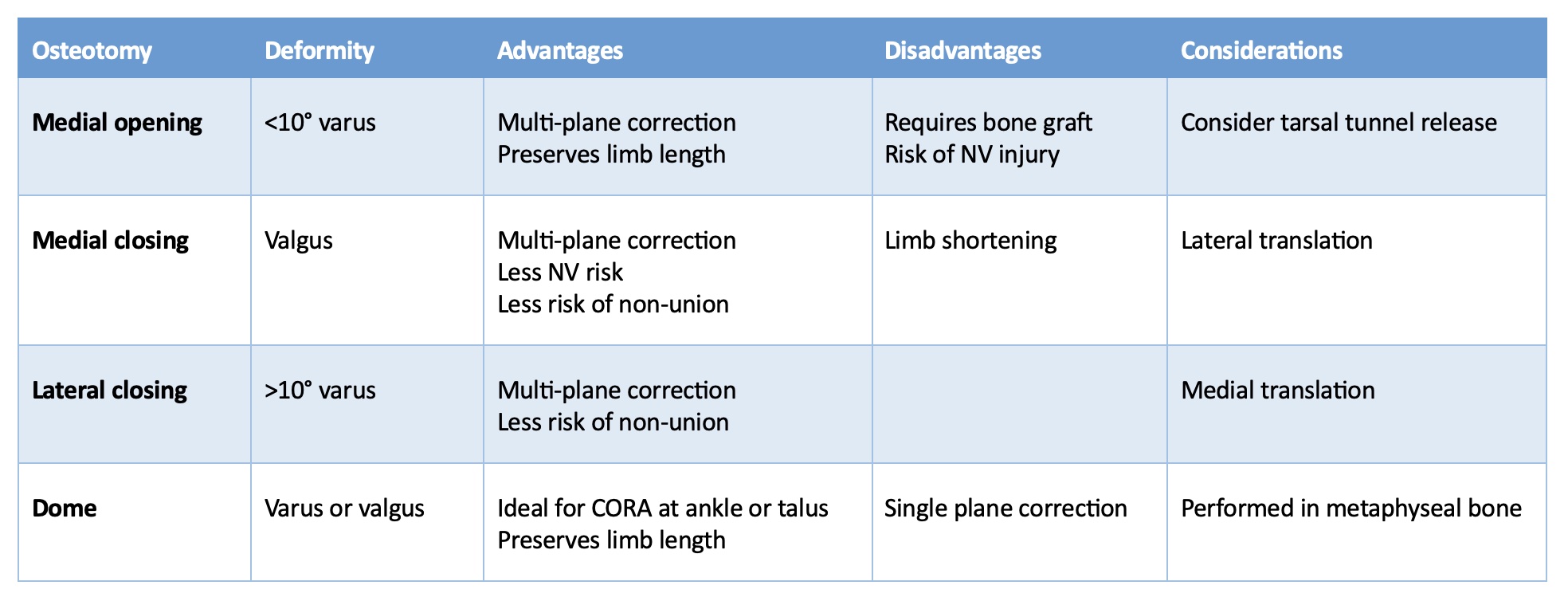
Table 1. Advantages and disadvantages of supramalleolar osteotomies
OPENING AND CLOSING WEDGE OSTEOTOMY
In general, for correction of varus or valgus deformity, use a half pin percutaneously placed as near to the CORA as possible in the distal metaphyseal region of the tibia to serve as the centre of rotation for the osteotomy. When the CORA falls at the ankle joint, the pin cannot be placed in the joint but can be placed just proximal, which will cause some translation. The osteotomy is performed in metaphyseal bone and the guide hole that is used is the one that will provide the ability for the osteotomy to exit both the medial and lateral cortexes of the tibia. Multiple holes are made along the planned osteotomy line and completed using an osteotome or saw blade to connect the holes.
Lateral closing wedge osteotomy
- 10 to 12cm longitudinal incision along the anterior margin of the distal fibula
- In most varus deformities, the fibula is also shortened; this is done with a bone block removal or Z-shaped osteotomy
- K-wires are drilled across the tibia, converging at the medial cortex; the osteotomy is performed and secured with a plate
- The fibula is secured with screws or plate
Medial opening wedge osteotomy
- Longitudinal incision along the distal medial metaphysis posterior to the great saphenous vein and nerve
- The tibia is exposed, preserving the periosteum
- Using fluoroscopy, a guidewire is placed from medial to lateral in the plane of the planned osteotomy
- The osteotomy is completed using a wide saw blade and the correction is made, typically preserving the lateral cortex to enhance the intrinsic stability
- The osteotomy is gently distracted using a lamina spreader and the space is filled with an appropriately sized bone graft
- In cases of sagittal plane deformity, an anterior or posterior medial wedge can be performed in a biplanar fashion
- Rigid plate fixation with locking screws is recommended to secure the osteotomy
- After the correction, the alignment of the heel is reassessed clinically; the aim is to achieve a heel with 1° - 5° valgus
- Lateral cortical fracture is less likely to occur when an opening wedge SMO is at the level of the proximal third of the syndesmosis, the so-called “safe zone,” rather than above (due to thick periosteum, syndesmosis, AITFL, PITFL)
Focal dome osteotomy
- Typically used for frontal or sagittal plane correction at, or near, the ankle joint
- An axis pin is placed in the distal tibial metaphysis at the CORA to avoid producing a secondary deformity
- A Rancho cube is used over the pin to allow circular rotation outlining the arc of the osteotomy
- The holes in the cube are drilled and connected with an osteotome
- An osteotomy of the fibula is then performed to allow mobilization of the distal fragment
- Strong fixation is needed for a rigid construct
Patient specific instrumentation (PSI)
- Many options now exist for PSI
- Based on pre-operative CT with a specific imaging protocol
- CT images sent digitally to the company, along with aims of surgical correction
- Patient-specific 3D sterile cutting blocks are produced by the manufacturer
- Aim is to reduce surgical time and increase accuracy of correction
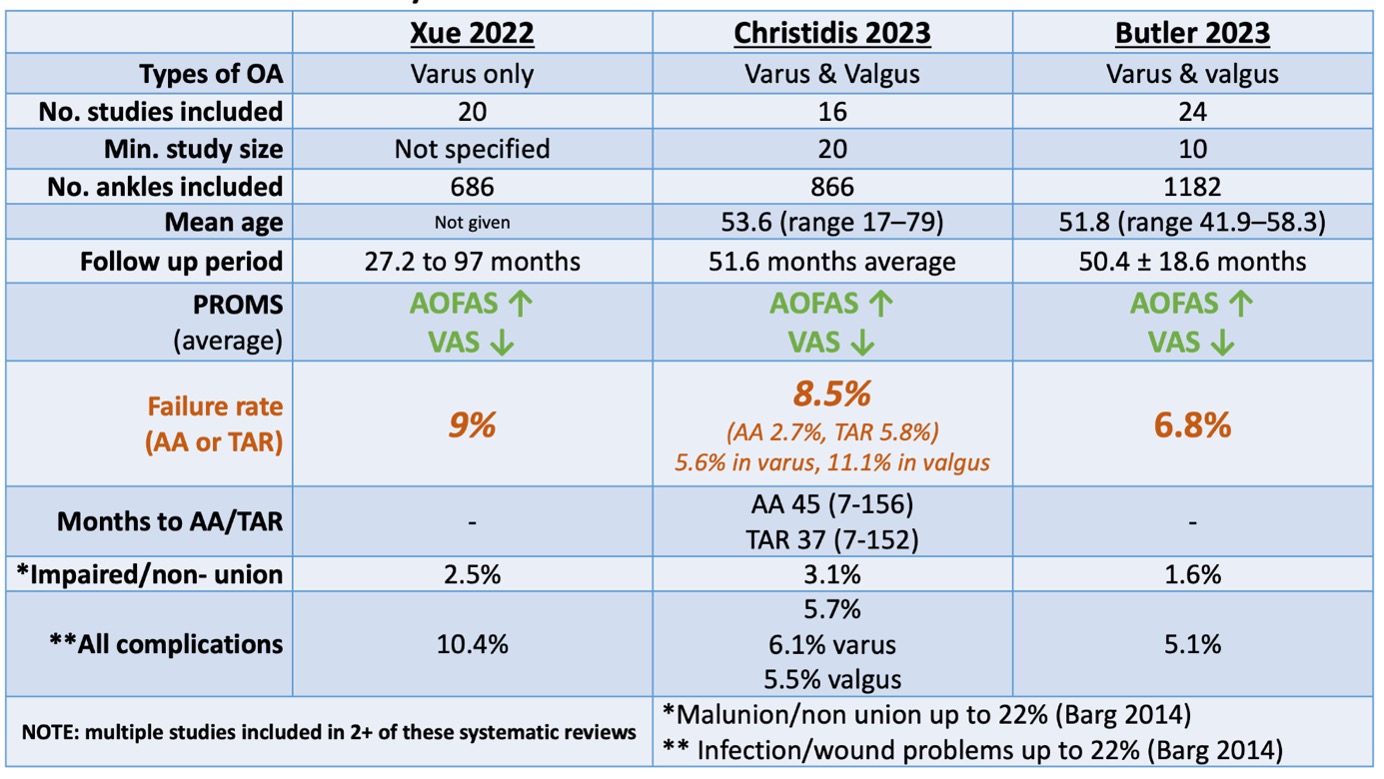
Complications
Although multiple studies have found substantial pain relief and functional improvement from SMOs, for both varus and valgus deformities, complications occur:
- wound healing problems and infections up to 22%
- malunion or nonunion up to 22%
There is little evidence that surgical technique, use of allograft versus autograft, or type of fixation affects union rates in distal tibial osteotomies. The progression of degenerative OA after SMO is reported to be up to 25% in the literature.
Outcomes
3 systematic reviews have shown failure rates of 6.8 – 9% at approximately 4 years
Comparative studies
There are very few comparative studies of SMO against alternative surgical management of ankle arthritis
- SMO vs. ankle arthrodesis (X-Q Yang 2022)
- retrospective review of 28 SMOT vs 30 AA at 50 months
- VAS and SF-12 physical marginally better in AA
- satisfaction better in AA
- complications similar
- reoperation higher in SMOT
- SMOT vs Distraction (ADA) (Z Yang 2022)
- ADA (32) vs SMO (41) Stage 3 post-traumatic varus OA
- 32 months FU
- AOFAS and VAS: no difference
- Complications similar
- Range of motion better in ADA
Complications
- wound healing problems and infections up to 22%
- malunion or non-union up to 22%
- significant re-operation rate
- progression of OA is up to 25%
There is little evidence that surgical technique, use of allograft versus autograft, or type of fixation affects union rates in distal tibial osteotomies.
Summary
- SMO has been shown to have good mid-term results in patients with mid-stage, asymmetric ankle arthritis and varus/valgus distal tibial deformity
- The primary indication for SMO is a deformity at the supramalleolar level
- Studies have shown it to be an effective option in avoiding joint-destructive procedures for ankle arthritis
- With proper patient selection and preoperative planning, the supramalleolar osteotomy can effectively redistribute the forces placed on the ankle, limiting progression of further degenerative changes and improving pain and functionality
References
Krähenbühl N, Akkaya M, Deforth M, Zwicky L, Barg A, Hintermann B. Extraarticular Supramalleolar Osteotomy in Asymmetric Varus Ankle Osteoarthritis. Foot Ankle Int. 2019 Aug;40(8):936-947. doi: 10.1177/1071100719845928. Epub 2019 Apr 25. PMID: 31023078.
Barg A, Saltzman CL. Joint-Preserving Procedures in Patients with Varus Deformity: Role of Supramalleolar Osteotomies. Foot Ankle Clin. 2019 Jun;24(2):239-264. doi: 10.1016/j.fcl.2019.02.004. Epub 2019 Apr 2. PMID: 31036267.
Hintermann B, Zwicky L, Schweizer C, Ruiz R, Barg A. The Use of Supramalleolar Osteotomies in Posttraumatic Deformity and Arthritis of the Ankle. JBJS Essent Surg Tech. 2017 Oct 11;7(4):e29. doi: 10.2106/JBJS.ST.16.00081. PMID: 30233964; PMCID: PMC6132995.
Krähenbühl N, Zwicky L, Bolliger L, Schädelin S, Hintermann B, Knupp M. Mid- to Long-term Results of Supramalleolar Osteotomy. Foot Ankle Int. 2017 Feb;38(2):124-132. doi: 10.1177/1071100716673416. Epub 2016 Oct 11. PMID: 27765869.
Hintermann B, Knupp M, Barg A. Supramalleolar Osteotomies for the Treatment of Ankle Arthritis. J Am Acad Orthop Surg. 2016 Jul;24(7):424-32. doi: 10.5435/JAAOS-D-12-00124. PMID: 27195382.
Yang, X.-Q., Zhang, Y., Wang, Q., Liang, J.-Q., Liu, L., Liang, X.-J., & Zhao, H.-M. (2022). Supramalleolar Osteotomy vs Arthrodesis for the Treatment of Takakura 3B Ankle Osteoarthritis. Foot & Ankle International, 43(9), 1185–1193.
Yang, Z., Cui, L., Tao, S., Zhao, J., Wang, L., Zhang, F., & Shao, X. (2022). Comparisons between ankle distraction arthroplasty and supramalleolar osteotomy for treatment of post-traumatic varus ankle osteoarthritis. BMC Surgery, 22(1), 178.
Butler, J. J., Azam, M. T., Weiss, M. B., Kennedy, J. G., & Walls, R. J. (2023). Supramalleolar osteotomy for the treatment of ankle osteoarthritis leads to favourable outcomes and low complication rates at mid‐term follow‐up: a systematic review. Knee Surgery, Sports Traumatology, Arthroscopy, 31(2), 701–715.
Christidis, P., Lampridis, V., Kalitsis, C., Kantas, T., Biniaris, G., & Gougoulias, N. (2023). Supramalleolar osteotomies for ankle arthritis: a systematic review. Archives of Orthopaedic and Trauma Surgery, 143(9), 5549–5564
Xue W, Chen T, Wahafu P, Li F, Xiahatai A, Wufuer A, Tuo Y, Zhao B, Wang C. Efficacy evaluation and systematic review of supramalleolar osteotomy for treatment of varus-type ankle arthritis. J Orthop Surg (Hong Kong). 2022 May-Aug;30(2)