Scarf versus Distal 1st Metatarsal Osteotomies
Introduction
Hallux valgus is a complex multiplanar deformity, due to various extrinsic and intrinsic causes, with a prevalence of between 23% and 36%. There are many surgical corrective options, from proximal to distal (see Table 1). Common adjuvant procedures include the Akin osteotomy and lateral soft tissue releases.
Hallux valgus can be graded as mild, moderate, or severe, based on the hallux valgus angle, the intermetatarsal angle and the distal metatarsal articular angle.
Typical practice in the UK, based on the severity of deformity, involves:
- Mild: chevron or short scarf osteotomy
- Moderate: scarf osteotomy
- Severe:
- proximal metatarsal osteotomy
- corrective fusion of the 1st MTP joint
- corrective fusion of the 1st TMT joint
Causes of recurrent deformity include:
- patient-related factors:
- e.g. Parkinson’s disease, high BMI, gout, hypermobility
- anatomic predisposition (e.g. pes planovalgus, joint congruence, pronated MT head)
- poor post-operative compliance
- Surgical factors include:
- procedural choice
- surgical / technical expertise
Recurrence rates can be as high as 50%, although often quoted as 5-10%.
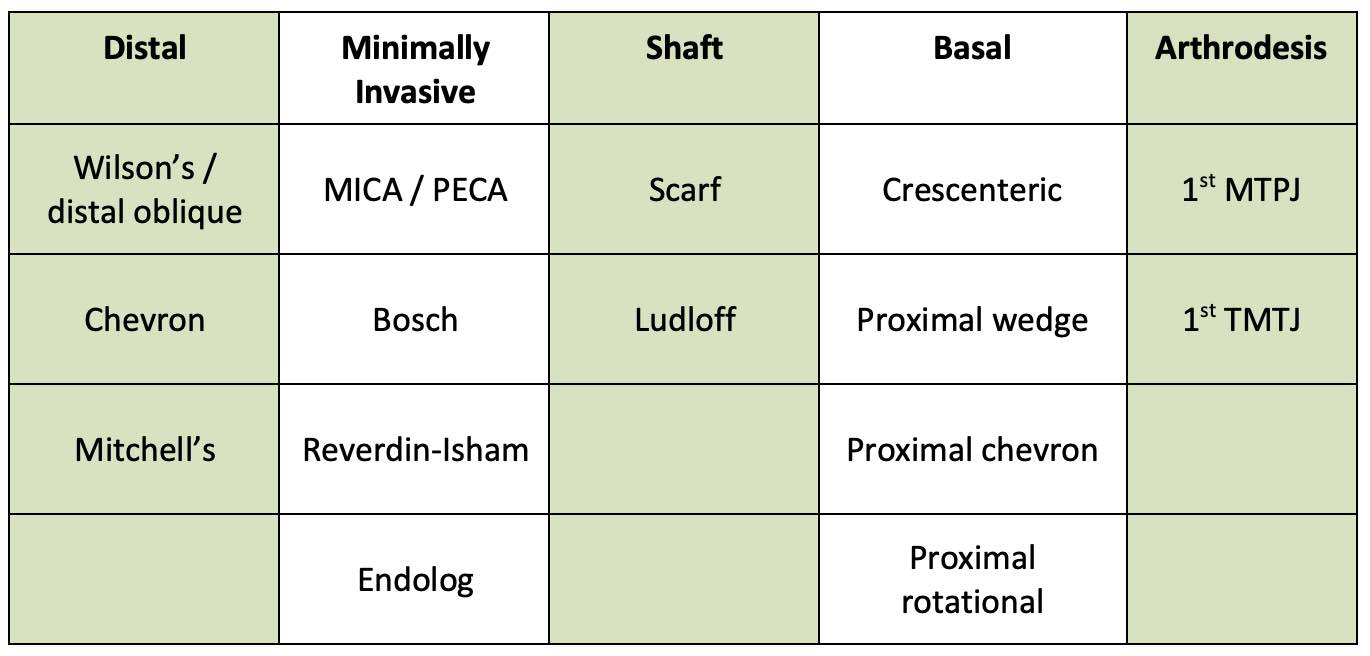
Table 1: Summary of open and minimally invasive procedures to surgically correct hallux valgus deformity (MICA = minimally invasive chevron-akin; PECA = percutaneous chevron-akin; MTPJ = metatarsophalangeal joint; TMTJ = tarsometatarsal joint).
Scarf Osteotomy
This is a a triplanar osteotomy involving a z-shaped cut to translate the distal fragment (figure 1). Due to its versatility, it can be used to treat a wide range of deformities as it can:
- laterally shift the first metatarsal
- lower or elevate the metatarsal head
- lengthen or shorten the first metatarsal
- provide axial rotation
Patient satisfaction and clinical outcome scores are excellent for most patients. Radiological recurrence rates have been quoted as around 10% but can be as high as 78% at 14-year follow up. Other complications include wound problems and nerve injury (~3%). Troughing, which is specific to scarf osteotomy, can be as high as 35%. The osteotomy is technically more challenging with a steeper learning curve compared to the distal osteotomies.
*Awaiting image upload*
Figure 1: The scarf osteotomy demonstrated in 2 views
Distal Osteotomies
*Awaiting image upload*
Figure 2: Examples of distal osteotomies
Chevron osteotomy
- most commonly used distal osteotomy
- shifts the distal fragment laterally initially described as being a symmetrical ‘v’, most now use a longer plantar limb to reduce the risk of avascular necrosis
- excellent outcomes in mild to moderate deformity
- good results in severe hallux valgus deformity
- less technically demanding than a scarf osteotomy
- complications (such as AVN and non-union) are rare
- radiological recurrence is normally quoted as around 10% but can be as high as 73% at 14 years
Less commonly used distal osteotomies include:
Wilson’s
Oblique metaphyseal osteotomy from distal medial to proximal lateral, allowing displacement of the metatarsal head laterally but with significant shortening
Mitchell’s
Double cut through the first metatarsal neck, leaving a step in the lateral cortex to ‘hitch’ the head on to the shaft. The head fragment is displaced laterally and plantarwards and held with a suture or screws. Good clinical results with 91% patient satisfaction in mild to moderate deformity.
After both Wilson’s and Mitchell’s osteotomies, shortening of the first metatarsal (3-7mm), transfer metatarsalgia (11-20%) and dorsal malunions are often a problem.
Minimally invasive surgery (MIS) for hallux valgus
Potential benefits include:
- reduced length of hospital stay
- quicker healing times
- reduced pain scores
- smaller scars
Complications include:
- thermal damage
- tendon injury
- disruption to local blood supply
- inflammatory reaction to bone debris
- 1st MT mal-positioning, shortening, or avascular necrosis
Initially, percutaneous hallux valgus correction was carried out using Bosch or Reverdin-Isham procedures or variants of these. Their popularity during the 1990s helped expand the use of MIS and paved the way for the development of newer techniques, including arthroscopy-assisted, the Endolog system, or percutaneous chevron-Akin osteotomies.
The Bosch method is a percutaneous, subcapital osteotomy under fluoroscopic guidance using a high-speed burr. A percutaneous K wire is used as stabilization for 6 weeks. Complications include stiffness in 31% and pin-site infection in up to 15%. Malunion rates can be as high as 50%.
The Reverdin-Isham technique is an oblique medial closing wedge osteotomy to the head. Studies have shown significant problems regarding transfer metatarsalgia and shortening. It is also difficult to correct the IMA through this method.
The minimally invasive chevron-Akin (MICA) – also known as the Percutaneous chevron-Akin (PECA) – is combined with a percutaneous soft tissue release and fixed with compression screws (figure 3). MICA has shown:
- satisfactory HVA and IMA correction
- 7% malunion
- 5% transfer metatarsalgia
- 1.5% superficial wound infections
- 94% patient satisfaction rate
- non-union up to 10%
- osteonecrosis seems to be more common than with open surgery
*awaiting image upload*
Figure 3: Intraoperative radiograph of MICA performed in a patient with hallux valgus deformity
The Endolog device is a curved, titanium endomedullary nail, which holds the lateral translation of the metatarsal head and does not require routine removal. It has shown excellent results and very low complication rates (up to 10%) in all studies.
When comparing MIS and open chevron surgery for hallux valgus correction, the clinical and radiographic postoperative scores are no different, but significantly improved, in both groups. There is a steep learning curve with MIS, which has led to some surgeons going back to open surgery. Studies have shown poorer radiological and clinical outcomes after MIS surgery in severe hallux valgus deformity.
Summary
More than 100 different operative procedures have been described to treat hallux valgus. Of these, the scarf or chevron osteotomy can be successfully used to treat the majority of deformities. The chevron is less technically demanding when compared to the scarf. MIS techniques may lead to better early function but with a higher complication rate. Individualised pre-operative assessment of patient factors, anatomic factors and surgical factors need to be considered during surgical planning.
References
Smyth NA, Aiyer AA. Introduction: Why Are There so Many Different Surgeries for Hallux Valgus? Foot Ankle Clin. 2018 Jun;23(2):171-182. doi: 10.1016/j.fcl.2018.01.001. Epub 2018 Mar 5. PMID: 29729792
Barouk L.S. Scarf osteotomy for hallux valgus correction. Local anatomy, surgical technique and combination with other forefoot procedures. Foot Ankle Clin. 2000
Jeuken RM et al. Long-term Follow-up of a Randomized Controlled Trial Comparing Scarf to Chevron Osteotomy in Hallux Valgus Correction. Foot Ankle Int. 2016 Jul;37(7):687-95. doi: 10.1177/1071100716639574. Epub 2016 Mar 23. PMID: 27009063
Robinson AH, Limbers JP. Modern concepts in the treatment of hallux valgus. J Bone Joint Surg Br. 2005 Aug;87(8):1038-45. doi: 10.1302/0301-620X.87B8.16467. PMID: 16049235
Malagelada F et al. Minimally invasive surgery for hallux valgus: a systematic review of current surgical techniques. Int Orthop. 2019 Mar;43(3):625-637. doi: 10.1007/s00264-018-4138-x. Epub 2018 Sep 14. PMID: 30218181
Clarke TAC, Platt SR. Treatment of hallux valgus by Scarf osteotomy - rates and reasons for recurrence and rates of avascular necrosis: A systematic review. Foot Ankle Surg. 2020 Aug 27:S1268-7731(20)30177-6. doi: 10.1016/j.fas.2020.08.009. Epub ahead of print. PMID: 32891491
MCQ
Which of these osteotomies can be performed through both open or minimally invasive approaches?
- Scarf
- Ludloff
- Chevron
- Mitchell
- Crescenteric
Which of these is NOT a risk factor for recurrent hallux valgus deformity?
- Pes planus
- Poor postoperative compliance
- Hypermobility syndrome
- Chevron instead of scarf osteotomy
- Parkinson’s disease